The right has a problem. It is not merely a Mitch McConnell or Kevin McCarthy problem. It’s a Republican Party problem. Conservatives will never have leverage to fight the issues that matter in any meaningful way until we find a new home. That is the stone-cold truth.
Before we can move forward, we must face this inconvenient reality.
No, a government shutdown has not been “averted,” because we now face the ultimate government shutdown — indefinitely — with no strategy or political vehicle to end it.
Republicans began this year with the most auspicious potential to block Joe Biden’s agenda. They had the twin leverage points of the debt ceiling and the budget deadline, whereby they could have refused to grant Biden any more funding for his harmful policies without serious concessions. In many respects, Republicans had more leverage than ever before because they could theoretically govern with a simple majority in the House while Democrats need 60 votes to use their majority in the Senate. Moreover, unlike during the tenures of Bill Clinton or Barack Obama, Democrats are saddled with an unpopular and inarticulate Democrat president who would not be able to command the bully pulpit during a shutdown fight.
So what happened?
Republicans in June gave Biden a blank check for the remainder of his term by suspending the debt ceiling until 2025 — more time than he had asked for. The debt has grown quicker than ever as a result.
The GOP’s final leverage point was the budget, and the intensification of the border invasion gave congressional Republicans the perfect mandate to fight through a government shutdown. Yet with both of these leverage points, Republican leaders showed that there is no degree of danger in which Biden can place this country that would prompt them to engage in brinksmanship. They wouldn’t even go up to the line and allow a lapse in funding at least for Sunday, when most government facilities are closed anyway. They fear one minute of a temporary funding lapse more than they fear crushing inflation, trillions in debt, millions of illegal aliens, and the FBI picking off political opponents.
I shudder to think exactly what it would take to shift Republican leaders’ attention away from the old paradigm. Everything we have been through these past few years was evidently not enough. It’s also shocking how Republicans had no problem shutting down the whole country for months, yet they zealously clamor to avoid one minute of a partial federal furlough over a weekend.
What’s clear is that nothing has changed about this party since the era of Trump began — not among leadership and not among the overwhelming majority of rank-and-file members. If they can’t fight even for a few days into a government shutdown over such popular issues and against such unpopular Democrat opponents, they will never ever fight for us.
We will now suffer through endless inflation, invasion, war on our energy and freedoms, and political persecution with zero backstop in sight. There is quite literally nothing Democrats can do that would elicit a unified, righteous response from the Republican Party. It’s not that they don’t have values — they certainly care deeply about funding Ukrainian oligarchs — it’s just that you and I are not part of their value system.
Not that we can even wait until 2025 to redress the aforementioned crises, but nothing will change then either — even if Republicans win all three branches. With such a maniacal degree of fear of a debt ceiling or budget funding lapse, Republicans will never have leverage to fulfil a single campaign promise, assuming any of those promises are even a little sincere. Democrats will always have enough votes in the Senate to filibuster any GOP budget bill. GOP leaders have made it clear that they will never allow the government to shut down for even one day. By definition, that means Democrats will always win a budget fight 100% of the time.
We need not speculate about the future when in fact this is what occurred when Republicans controlled the trifecta of government with Donald Trump as president, McConnell as Senate majority leader, and Paul Ryan as speaker of the House. As I noted earlier this year, Kevin McCarthy was House majority leader and shepherded nearly every budget bill through the floor with more support from Democrats than Republicans. Nothing has changed, and nothing will.
But it’s worse than the political math at the federal level. In more than 20 states, Republicans enjoy control of all three branches with filibuster-proof majorities. Why is it that we can barely find Republicans outside Florida willing to fight on issues such as “green” energy and illegal immigration? They wield dominant majorities — in some states to the point where there aren’t enough Democrats to populate all the committees! Yet Republicans still betray us. At some point we have to face the music that the obstacle to reform has nothing to do with the media or the Democrats. The Republican Party is the problem.
We are now 2+ years into consuming reams of information showing the vaccines were devastating to humanity. What will Republicans do about it other than whine about censorship? Refusing to focus on vaccine injury and the perfidy of the government-vaccine complex is an act of self-censorship.
There is a bizarre dynamic unfolding as it relates to GOP sentiment toward the vaccine. All Republicans recognize and decry the growing evidence of the government’s collaboration with big tech to censor all information about vaccine injury. Yet they seem to be more upset about the censorship of the information than about the information itself. Why is there no push from Republicans to defund the vaccines and fix the regulatory and legal structures that allowed Operation Warp Speed to occur and that continue to gaslight the next iteration of rushed, dangerous vaccines?
In an extraordinary ruling on Independence Day itself, Louisiana federal Judge Terry Doughty issued a broad injunction against all government agencies on working with social media companies to censor politically unfavored speech. Citing “substantial evidence” of government’s “dystopian” violations of the First Amendment, Judge Doughty prohibited the federal government from “encouraging, pressuring, or inducing in any manner the removal, deletion, suppression, or reduction of content containing protected free speech.” The injunction not only includes the HHS agencies censoring COVID information, but also the FBI, the Cybersecurity and Infrastructure Security Agency, the State Department, the DOJ, and the White House censoring all forms of protected speech.
This ruling comes a week after the House Judiciary committee produced a preliminary report showing DHS’ CISA was behind the censorship enterprise. It turns out that CISA funded a nonprofit group to work with social media on a process, known as “switchboarding,” which would “trigger content moderation” to “ensure priority treatment of misinformation reports.”
Republicans seem united in combating this censorship and plan to include provisions in the relevant appropriations bills for fiscal year 2024 to block funding for these surveillance and censorship programs. However, where is the same degree of outrage about the dangers of the vaccines themselves?
We now have over two years of information showing ubiquitous injury stemming from damage to all parts of the body, particularly cardiac and neurological. Whether it’s VAERS, European data, countless independent studies, epidemiological data, excess deaths and “died suddenly” mysteries correlating with the take-up of the vaccines, health insurance data, life insurance data, or disability data – we have enough evidence to convict this shot for murder if it were a human standing for trial. Yet not only have these vaccines not been defunded, the same framework that rushed their approval has already been used for countless other new vaccines.
The government’s new shell game is to concede the existence of these problems, but play semantics with the term “rare” when describing their risk. Science Insider published a piece acknowledging the “rare link between coronavirus vaccines and Long Covid–like illness,” including blood clotting, heart inflammation, and neurological disorders. Even Peter Marks, the man at the center of Operation Warp Speed, admitted, “We can’t rule out rare cases.”
“If a provider has somebody in front of them, they may want to take seriously the concept [of] a vaccine side effect,” admits the director of the FDA’s Center for Biologics Evaluation and Research, two years after emails show he ignored concerns of rushing the vaccine amidst a pileup of adverse event reporting.
However, what is rare? The CDC’s own pharmacovigilance program showed a 7.7% rate of clinical-level injury. Coupled with the underreporting rate in VAERS, there were likely millions of severe and long-term injuries, including several hundred thousand deaths in the U.S. So yes, we can suggest that 92% of people didn’t experience clinical levels of injury and 98%-99% didn’t experience long-term and deadly injuries. In that sense, I guess you can say it’s rare. But how many people are we talking about when 5.5 billion people were given at least one dose? Potentially, millions of deaths and hundreds of millions of injuries! Just consider the fact that 25% of injuries reported to VAERS and about a third reported by the European Medicines Agency are considered serious, well beyond the standard of 15%.
House Republicans can no longer ignore the problem with the vaccines. They must also stop ignoring the endless approvals of monkeypox and RSV shots based on dubious data and the same rushed framework. To that end, Speaker McCarthy should take the following actions.
Create a commission of members of Congress to examine the rationale, safety, and efficacy data of all vaccines, beginning with the new ones recently approved and in the pipeline.
Bar any involvement in a WHO pandemic treaty or expansion of the International Health Regulations.
Repeal immunity for vaccine manufacturers, including the provision in the 21st Century Cures Act of 2016 that extends the immunity to vaccines offered to pregnant women.
To this day, we still can’t get Republicans to shake their support for the V-word even in red states. Last week, Ohio Gov. Mike DeWine, the consummate COVID fascist governor, used his line-item veto to strike a provision from the budget ending vaccine mandates in colleges. “University and college dormitories and student housing are congregate settings where such policy may be of great importance to ensure resident safety,” said DeWine of vaccine mandates in his veto message. It takes a new level of cognitive dissonance to support mandates on those who don’t want the shot out of fear of harming those who did supposedly get the protection that evidently fails to protect unless the other person gets it!
Republicans all agree that our government engaged in an unprecedented operation to cover up the truth about vaccines. How come their curiosity stops at the degree of exposing the cover-up with no interest in delving into what exactly they are trying to cover up? After all, this is the only product that automatically goes into every arm of every baby multiple times after birth with a set schedule mandated by schools. Certainly the COVID shots are proven to be poison, but is there no interest in uncovering the broader truth?
Editor’s note: This article has been corrected to note that 5.5 billion, not 5.5 million, received at least one dose of a COVID vaccine.
Like Blaze News? Get the news that matters most delivered directly to your inbox.SIGN UP
“Justice is indiscriminately due to all, without regard to numbers, wealth, or rank.” ~John Jay, in Georgia v. Brailsford, 1794
The die is cast. The political persecutions have been happening against average conservative citizens for several years, but it took the indictment of Trump to finally get people’s attention. We no longer have equality under the law. It’s quite evident that a conservative living in a blue state or being prosecuted by the feds in D.C. will never get a fair shake from the prosecutor, judge, or jury. Nothing will change that. The question is whether red states will make their states sanctuaries for liberty and as unhospitable to their political enemies as blue states are to our people.
It wasn’t always this way. We’ve been an extremely divided and polarized nation for quite some time. Sure, in the realm of court decisions or the legal process affecting broad political issues, the political bias of the judges was always quite apparent. But when it came to an individual criminal case, it was always the law that governed. As recently as 2016, a unanimous Supreme Court vacated the conviction of former Republican Governor Bob McDonnell for bribery because they all clearly understood that the governor’s hosting of a company he benefited from, while reeking of sleaze, is endemic of both sides of the political divide and clearly did not meet the definition of bribery under the Hobbs Act.
We no longer live in a world of equal justice under the law. We’ve witnessed how in the same capitol city where violent criminals are released or not prosecuted, Army veterans with clean records were held pretrial and denied due process up and down the legal system on what was, at most, non-violent misdemeanors, and at worst government provocation and entrapment. All of this is taking place while the worst Antifa rioters can take over city streets for weeks with brutal violence. Aside from Elizabeth Warren’s isolated moment of intellectual honesty decrying solitary confinement for J6 defendants, we’ve seen no such outcry for equal treatment. Those perpetrating this believe we are subhuman and not afforded equal protection under the law.
Some countries are open and anarchic like places in the Third World; others are very authoritarian like Singapore, where everyone is punished pretty severely for relatively minor infractions. But what we have here is a two-tiered justice system that is tantamount to targeted and systemic persecution. This is how we wind up with D.C. U.S. Attorney Matthew Graves refusing to prosecute 67% of all arrests, including 52% of all felonies, but announcing 1,200 new prosecutions of J6 protesters, many of individuals who didn’t even violate minor trespassing laws. This is how you have endless Antifa and BLM riots where the most violent people who beat, maimed, looted, and burned police stations to the ground got less punishment than the most innocuous J6 suspects.
We cannot share a country with people who don’t fundamentally believe in equality under the law. This was self-evident before the Trump indictment, and frankly, it’s shameful that so many conservative voices didn’t respond emphatically to this emergency until it affected their man. Nonetheless, if this is what it takes to unite behind a forward-looking agenda, we’ll be better for it. Thus, the only answer is to militarize the legal system of red states just as emphatically as blue states. To that end, red state governors and legislatures should do the following:
1) Fund legal defense of persecuted individuals: The first step is defense. Obviously, Trump has a war chest, but most of his supporters being persecuted or pro-life activists being targeted for praying outside abortion clinics don’t have money. It’s also extremely hard to even get a lawyer willing to fight the system. I personally had trouble finding people lawyers when fighting January 6 charges or businessmen being prosecuted for the “crime” of opening their stores during COVID. Red states should set up a legal defense fund to contribute to the legal defense of those the state AG determines are being targeted with unequal treatment based on political, religious, or social beliefs. The AG’s office can also marshal pro bono lawyers willing to help who know that they will get moral support from the state rather than being targeted as pariahs in their profession for representing such clients.
2) Refuse to extradite: Gov. DeSantis just set a precedent that Florida will not assist with extradition of those politically targeted. Other red-state governors should refuse to extradite people being accused of non-violent crimes when there is compelling evidence that other people accused of similar actions are not targeted with the same level prosecution. In the case of Trump, because he is protected by the Secret Service, there was never a chance that the NYPD would somehow be able to nab him in Florida. But for ordinary citizens, it’s important for red states to make the statement that they will serve as constitutional sanctuaries for equality under the law. This will be harder to pull off in the face of a federal prosecution, but the time has clearly come to tell the blue states to shove it. Every red-state legislature should empower its state AG to block extradition if he determines it is for political reasons.
3) Slash the ABA monopoly: Connected to the previous point, it’s time for state legislatures to require their state judiciaries to recognize alternatives to the American Bar Association, which has unlawfully claimed a monopoly on the entire legal profession to the point where people cannot obtain legal representation over the ABA’s veto. The ABA is sanctioning people like Rudy Giuliani and Professor John Eastman for simply offering their view on constitutional questions.
4) Refuse cooperation with rogue federal agencies: Red states need to pull out of all joint training, sharing of information, and help with logistics or intel to any federal law enforcement agency that continues to target people for their political beliefs.
5) Prosecute the left more zealously: It’s time to fight fire with fire. Just this week, there was a left-wing insurrection at the Tennessee Capitol. We’re not asking red-state prosecutors to take minor misdemeanors and hold people pretrial for two years as the left has done with J6 defendants. However, they should more aggressively use catch-all felony statutes to throw the book at people who legitimately act violent or Democrat politicians and outside groups that legitimately violate laws.
Even though they don’t control the federal government, Republicans control half the states and can easily make these changes today. That’s why the primary focus should be interposing on behalf of the people’s liberties at the state level. However, given the federal tyranny, there is a need to at least push for legal reforms against political targeting with legislation in the House.
6) Pass the “Political Targeting Prosecution Act”: Defendants can theoretically assert an Equal Protection Clause violation; however, practically, the courts have made it almost impossible to succeed in a claim of a selective prosecution defense under the Equal Protection Clause. As such, Congress should pass the Political Targeting Prosecution Act, which would accord defendants the opportunity to present evidence of political targeting based on animus for the individual’s religious or political beliefs. For example, if defendants could show how no BLM rioter who was much more violent was charged with obstructing law enforcement during a public disturbance (18 USC 231(a)(3)), it would trigger a motion to dismiss based on unequal treatment.
7) Fair jury pools: With a country more divided than during the Civil War, it’s self-evident that conservatives cannot get a fair trial in liberal jurisdictions. This has rendered the Sixth Amendment’s guarantee to a trial by a jury of one’s peers irrelevant. In order to restore the spirit of that right in this era, Congress must demand that a conservative defendant charged in D.C. can move the trial to the federal jurisdiction where the defendant resides. There should also be a federal right to request an expanded jury pool 20-30 miles outside a major city to obtain a more “equitable” share of like-minded people composing the jury in criminal cases. So for example, whenever Democrats control the Justice Department, by definition, any political opponent will be charged in D.C. with a 95% Democrat jury pool. The new law would prescribe that the individual is tried either in his home state or, if he resides in D.C., he could request a jury pool to rope in parts of Maryland, Virginia, and the West Virginia panhandle to achieve more balance.Trump fans are absolutely correct in asserting that this is about much more than Trump. Indeed, the political persecutions have been going on for quite some time before this indictment. So let’s make our response about more than Trump and more than just promoting talking points. It’s time for action. Let’s systemically combat the weaponization of the justice system against those who have no voice, money, or legal help.
Nobody disagrees at this point that there is a plethora of excess deaths and a dearth of births, a trend that should be the number-one alarming public policy issue. Yet when any of us suggest that the gene therapy ubiquitously given to the world right around the time of the jump in these numbers might be responsible, people look at us like we are from Mars. However, it turns out, based on newly released FOIA documents from the CDC, that our government knew about and even anticipated massive reports of injuries from these shots from day one.
Throughout the past two years, the government and media have concocted a conspiracy theory that somehow the CDC’s own VAERS reporting is scammed with fraud by people who have nothing better to do with their lives but spend hours filling out fraudulent vaccine injury reports. They pretend it’s a sort of ex post facto anomaly that nobody expected and that has no credibility in their eyes. Except, as Hebrew University Professor Josh Guetzkow reveals, not only did the CDC know about the vaccine injuries blowing up VAERS at record levels (even before the general public had access to them), the agency contracted with defense contractor General Dynamics to handle the database in anticipation of record use. Then, when the vaccines were released, the CDC had to up the contract to account for even more entries, yet showed no moral qualms about continuing with the campaign without disclosing these revelations to the public.
Guetzkow, who has secured numerous FOIA’ed documents both in the U.S. and Israel throughout COVID, posted 69 pages of FOIA’ed documents and contracts from General Dynamics Information Technology to the CDC’s immunization safety office. Thanks to his work, we already know from the previous FOIA’ed documents that the CDC’s $9.45 million contract with General Dynamics in August 2020 stated that officials anticipated 1,000 adverse event reports a day, with 40% of them being serious. Yet, like a cold serial killer soullessly counting his casualty list, the CDC was completely fine with going through with this campaign, as if it were the price that had to be paid to worship the spirit of the age – the modern-day Moloch. However, this document shows that as early as Jan. 15 – when most people still could have avoided these shots – the CDC was aware of record-setting reports that crushed even the agency’s initial cold-hearted, morbid expectations.
As you can see from page 8 of the pdf, General Dynamics warned the CDC that VAERS had blown through the expected 1,000 cases per day and even reached a level above 4,500 – to the point that GD couldn’t process the data. Mind you, they were never concerned with the human toll, just the logistics of the contract labor. They predicted a need for “reforecasting of staffing needs” to process all these reports.
Already in December 2020, when the shots were only available for select people like doctors, there were over 19,000 reports and close to 344,000 website visits. It’s hard to see how this wasn’t organic from people genuinely in pain because there was no organized campaign in the United States to inform people of VAERS at the time. I myself (who obsessively focused on this) hadn’t heard of it until two months later.
By Feb. 15, General Dynamics reported a continued record-setting pace of reports and website visits, to the point that workers had to expand their VAERS ID reports to allow for seven digits instead of six. In April, officials reported that they had to hire an additional 200 staffers to deal with the backlog and continue to process 25,000 reports per week, well beyond the threshold they originally contracted for. As eligibility for the shots expanded for all age groups, they continued to process over 30,000 injury reports a week, yet the CDC never said a word about it. Not only did officials not take the products off the market, they began mandating them over late summer 2021, with some mandates that remain in place to this very day.
It’s nearly impossible to astroturf these sorts of injury reports. Clearly, our government saw how organic they were and how they coincided perfectly with the uptake of the vaccine. Indeed, the FDA had access to the infamous Pfizer document in Feb. 2021 – before almost any younger adult was vaccinated – showing that the shot killed over 1,200 people and was associated with over 1,400 categories of serious maladies that were chronicled in a list eight pages long.
Now, keep in mind that after the government observed all these adverse events, and after officials knew about the 7.7% clinical injury rate from the CDC’s own V-SAFE program, perfectly corroborating the VAERS data, they accelerated the approval of these shots for children and then the mandates for everyone. Emails released via FOIA show that in July 2021, when the shots should have been canceled, Peter Marks, head of the FDA’s Center for Biologics Evaluation and Research, pressured Marion Gruber, then head of the office of vaccines research and review, to truncate the already accelerated timeline to fully approve the Comirnaty shot (which is still not commercially available 2.5 years later).
A copy of the July 19 email response from Marion Gruber is below:
A week after the infamous Aug. 23 approval, which triggered the mandates, Gruber resigned from the agency in protest. But notice how even Gruber couched her reticence to approve this thing in terms of not undermining “confidence in the vaccine,” rather than expressing actual concern this was already killing and maiming people in droves.
We’re at the point where at a minimum, the government doesn’t care how many people die from this experimentation. Dr. Tom Merritt, who was part of the Oxford University team who developed the AstraZeneca vaccine, best summed up the sentiment of the biomedical state toward the people when he admitted that those injured by the gene therapy were “collateral damage to the bigger scheme.” He added: “Some tragically died, a number had their lives changed forever. They believed in vaccines; now they don’t.”It’s all a matter of what the bigger scheme really is.
Like Blaze News? Get the news that matters most delivered directly to your inbox. SIGN UP
We have no free market and never will have one so long as the Federal Reserve exists in its current form. It is the unelected judge, jury, and executioner of the economy that can pick winners and losers by manipulating credit and monetary policy to artificially inflate certain investments and investors at the expense of others. Years of unnaturally low interest rates have enriched well-connected woke elites at the expense of consumers and savers. Now that their Ponzi scheme is coming due, with the collapse of one of the wokest banks and the vicious cycle of stagflation and reliance on loose money, it’s time for conservatives and GOP presidential candidates to revisit the idea of either abolishing or severely limiting the role of the Fed.
For the past several generations, the Democrat Party thrived on class warfare. Democrats claimed that conservatives elevated the wealthy at the expense of the working class simply because they didn’t support free stuff and redistribution of wealth through an extremely progressive income tax on legitimately earned wealth. But it turns out that their policies have actually artificially enriched the wealthy and harmed middle-income consumers and savers, but unlike with our policies, the wealthy never earned these tendentious favors, nor are they constitutional.
In many respects, the Federal Reserve has more power than all three branches of government put together, yet the members never stand for reelection. For years, the Federal Reserve has created endless inflation and loose credit with near-zero interest rates and by buying up trillions of dollars of securities and treasuries. It distorted the market, allowed woke banks like Silicon Valley Bank to overextend themselves, and even become the primary lender for solar financing in America, based on Monopoly money.
Now that the Fed inevitably was forced to hike interest rates to curb some of the historic inflation it helped create, Silicon Valley Bank, along with Signature Bank in New York (the bank Barney Frank joined when he left Congress), collapsed and was taken over by the FDIC. But just like a frustrated teen losing a video game, the Federal Reserve and the Treasury Department are pulling the plug on the game so that their buddies don’t lose. Remember, until Friday, SVB’s CEO, Gregory Becker, was on the board of directors at the San Francisco Fed. It’s one big game of, by, and for the politically connected venture socialists.
Less than 10 hours after Treasury Secretary Janet Yellen promised there would be no new bank bailout, the Federal Reserve issued a statement Sunday evening announcing a spectacular bailout of every penny of deposits both at SVB and at Signature Bank. Except this one, unlike in 2008, won’t even require a vote in Congress, because the Federal Reserve and the Treasury Department have the backhanded tools to print money, even though we have reached the statutory debt limit.
“The financing will be made available through the creation of a new Bank Term Funding Program (BTFP), offering loans of up to one year in length to banks, savings associations, credit unions, and other eligible depository institutions pledging U.S. Treasuries, agency debt and mortgage-backed securities, and other qualifying assets as collateral,” wrote the Fed. “These assets will be valued at par. The BTFP will be an additional source of liquidity against high-quality securities, eliminating an institution’s need to quickly sell those securities in times of stress.
In other words, they are back to printing money. The Fed has already grown its balance sheet by $4.7 trillion during the frenetic COVID money-pumping scheme (in addition to Congress’ $5.5 trillion fiscal stimulus), and has only off-loaded roughly $600 billion over the past year.
This was after many preceding years of ultra-loose monetary policy. Finally, as inflation reached record highs last year, the Fed began to ease up on those policies. Not any more! The Fed is promising to buy the assets “at par,” not at market value, which will have the effect of loosening bank credit beyond belief.
Additionally, along with the Treasury Department, the Fed will make $25 billion available as a backstop to this quantitative easing scam. The debt limit is a complete mockery, because evidently the Treasury Department can come up with vast sums of money on the fly, and this is likely the tip of the iceberg. Once the initial shock of this policy sets in, the debate will merely be over how many hundreds of billions are offered to stem the panic from other banks.
The immediate effect of this bailout will be to halt all interest rate hikes. As of this morning, the yield on the two-year Treasury note was down more than 80 basis points since last week, in anticipation of the return to loose credit. So the government will crush consumers with record inflation to bail out the well-connected woke (ESG-supporting) elites who took advantage of the unnatural and manipulated easy credit. John Edwards was indeed correct that there are two Americas, except it’s not because of a lack of government involvement. It’s because of too much big government, and particularly an unelected fourth branch of government that should be abolished.
If it’s impractical to immediately abolish the Federal Reserve, we should at a minimum remove its power to serve as both the arsonist and the firefighter. Congress must repeal the Humphrey-Hawkins bill from 1978, which empowers the Fed with a “dual mandate” to achieve maximum sustainable employment and keep prices stable. The Fed should be forced to focus solely on price stability. This would take “the game” out of the Fed. If it has no ability to create stimulus and provide monetary morphine, Wall Street can’t anticipate it and build an artificial economy based on its nourishment.
Market-distorting monetary manipulations are no different from market-distorting fiscal policy from the government. This is how the statists have successfully dissuaded us from ever limiting government. “You really plan to pull the rug out from under such-and-such industry?” the forces of special interests groan, be it health care or the financial sector. The same applies to monetary policy. There is no reason why we should allow the Fed to use monetary stimulus in such an officious manner that the entire market would collapse without the monetary morphine, even during robust economic growth.
The Fed should also be banned from buying up other securities and bonds, such as mortgage-backed securities from Freddie and Fannie. We must stop distorting the markets by encouraging investments on the basis of how much capital is available instead of real growth in a specific industry. It’s time to go back to the days of real economic growth built on the fiscal equivalent of protein and healthy fats, not sugar and carbs for the well-connected elites involved in regulatory capture.
We have enough lawless, unelected branches of government. It’s time to stop creating asset bubbles and misallocation of resources and return to a true organic equities market that reflects the economic realities of America. That will not happen until the Fed is brought under the checks and balances of the republic. As Andrew Jackson warned of a central bank, “The bold effort the present (central) bank had made to control the government … [is] but premonitions of the fate that awaits the American people should they be deluded into a perpetuation of this institution or the establishment of another like it.”
The more money our government has pumped into cancer research, the more cancer has proliferated, culminating over the past year or so in an explosion of sudden cancers. We’ve spent $90 billion on cancer research just through the National Cancer Institute from 1971 until last decade. Yes, surgical techniques and early detection have gotten better in making certain cancers more survivable, but why have cancers exploded, and what about the progress and prudence of the standard oncological treatments? Are they really backed by data, science, and the good of the patient or by pharma greed and incentives created by government-funded monopolies, just as we saw with COVID?
This appears to be some of what is vexing the first lady of Florida in pursuit of her new approach to cancer funding, following her personal bout with breast cancer in 2021. “The Cancer Connect Collaborative will analyze and rethink the way Florida approaches cancer research, diagnosis, and treatments — through incentivizing proven and promising approaches to cancer care while reducing the role of bureaucratic red tape and special interests,” said Casey DeSantis during a public roundtable with Florida’s Surgeon General Dr. Joseph Ladapo and other local doctors. “This collaborative will chart a course of action that will lead the nation and ultimately save lives.”
Typically, federal and state politicians outbid each other in funneling money toward cancer research and treatment that just perpetuates the same failed status quo and likely empowers the same monopoly stifling innovative thinking and approaches. After all, who will oppose a proposal for more cancer research? But this $170 million initiative called the Cancer Connect Collaborative, a large sum of money for a state government, seeks to break down barriers to introducing new ideas.
It all begins with honesty. “We know a lot about cancer – what causes it, and in many cases, what preventative steps can minimize the risk of a diagnosis,” reads the one-page printout from the Collaborative. “It’s time to open the tap on cancer information, and the Collaborative will be tasked with identifying the ways to ensure this is done.”
The Florida first lady passionately asserted, “It’s not good enough any more to hear ‘we don’t know what causes cancer.’ We do know a lot of what causes cancer. And frankly, I would like that information laid out in a straightforward manner free from tainted influences. I’d rather not rely on content and random articles brought to you by special interests that may, unfortunately, be part of the problem.”
Many Americans have long surmised that Big Pharma has kept the “tap of information” on cancer closed to purposely perpetuate a model that maximizes revenue while achieving very uneven and questionable outcomes, often at the cost of the quality of life of the patient. It’s almost like the medical establishment is enjoying this too much. With cancers exploding across the country, we need state governments to start rethinking our approach to cancer and imposing more transparency and direction on the funding rather than a blank check. We must ask why cancers are exploding, what some of the potential causes are, and whether the current regimented way of treating it is really the best approach for humanity.
I’ve witnessed the difficulty and sorrow of many friends and family members going through various forms of cancer treatment in recent years. What is striking about this experience is that the oncologists almost appear to have a computer-based algorithm on how they treat patients. The cost-benefit analyses are already baked into predetermined formulas, and they don’t appear to update them with clear data and clinical outcomes or changing facts on the ground. They are obdurately conditioned to strict, robotic protocols.
What many of us have learned from COVID is that the government-pharma complex is willing to push dangerous and ineffective treatments on patients while actively stifling much safer and more promising alternatives. As such, does anyone really think there is no better approach to cancer than the current circulation of endless forms of chemo that are fueled by the data provided by the manufacturers themselves, not necessarily real-life outcomes? Remember the 95% efficacy of Pfizer’s shot? Do you really think that was the company’s first rodeo manipulating its trial data? At some point, outcomes need to matter.
To that end, DeSantis and Ladapo are promising to gather state data about the proliferation and treatment of cancer to make it “both timely available and easily accessible.” The key is to actually have trustworthy and timely data on the cancer rates and reoccurrence rates. Without that we cannot assess the efficacy of this pharma empire, which often accounts for the bulk of revenue for some companies and many medical specialties.
“Currently, there is about a two-year lag between the time the data is collected, submitted, and analyzed. We need real-time data to asses current trends … for example, why are so many types of cancer skewing younger and becoming more prevalent? Case in point [referring to her own experience]. Why are there increasing concerns recently from some physicians about higher rates of reoccurrence?” said Casey DeSantis.
Indeed, one of the lessons we should learn from the broken health care system in the wake of COVID is that you can’t properly treat something you fail to diagnose and asses in terms of its cause.
This was the problem from day one with COVID. At least 95% of doctors were flummoxed by COVID, but there were certain doctors, such as Drs. Brian Tyson and George Fareed in El Centro, California, who were clearly treating thousands of people in their urgent care with success. Why didn’t the medical establishment observe what they did and break the barriers for their successes to become a part of the standard of care elsewhere? We now know why this was the case with COVID, but who’s to say this isn’t happening to some degree with cancer treatment too?
Funding for cancer is always a double-edged sword. As we saw with COVID, the funding for treatment fueled terrible products and was used to actively ensure that no effective product would ever emerge or be promoted. Despite our medical system spending $600 billion a year on cancer treatment, double the per-person rate of the average of other wealthy countries, there is no evidence of meaningfully better outcomes, according to a recent study published in JAMA.
The fact that this cancer funding is being inaugurated under the watch of Dr. Ladapo, a man who recognizes the lessons of the COVID disaster, should give us more confidence that he will take the approach to cancer in a different direction, just as he stands alone on the COVID shots.
Ladapo, during his remarks, spoke about the need to “step out” of the typical threshold standards of the NIH for preliminary research needed to fund a clinical trial. As we’ve all witnessed, that standard is often used as a gatekeeper to keep out promising treatments while green-lighting problematic ones. Ladapo spoke of his own experience as a researcher in how he plans to use some of this funding to offer entrepreneur scientists who might not be connected wit the heavy-hitter pharma companies to prove the promise of their innovative research and ideas.
Also, in what sounded like a clear understanding of the lessons of COVID, Casey DeSantis called for the group to study all the “best practices” across the nation and state to see what works and why it’s not being done everywhere. “Why, if a physician has been utilizing a proven technique within their hospital system for years, and that successful procedure is not available to other patients across the state – if not, why not? What reasons or barriers to entry are prohibiting successful practices from being made available to Floridians? Is it bureaucracy? Is it the lack of a billing code that allows for reimbursement? …How does one treatment get the reimbursement green light, while others may not?”
Put another way, is the remdesivir vs. ivermectin dynamic also playing out in cancer research and protocols? Overall, DeSantis was motivated by her personal experience to ensure that others have clarity and the best options headed forward. “I have to admit this is not a subject that is very easy, as you can imagine, for me to talk about. But I’m of the mind [that] when much is given, much is expected. And if I have the opportunity … to put a lot of really smart people into a room to rethink the way we approach cancer care, I’m going to do it, even if I have to use the C-word now and again.”
According to new provisional data from the Scottish government, there were 7,314 deaths registered in January 2023, an increase of 17.7% compared to the average of 6,212. For the second week of January, there were more deaths in Scotland than ever before, including during the peak of the pandemic. Concurrently, there were 4,159 births registered in January 2023, a decrease of 6.8% compared to the average of 4,463. In other words, between a dearth of births and a plethora of deaths, there were roughly 1,400 fewer souls, the equivalent of roughly 86,000 in the United States. This is long after COVID. Why is there zero concern?
What on earth will it take to pull these death shots from the market?
Die Welt, a paper based in the home country of Pfizer partner BioNTech, revealed last week in a long expose what many of us have long known. All those sudden deaths, heart attacks, and strokes we’ve been witnessing over the past two years were indeed observed during the Pfizer clinical trial that supposedly showed the shots to be 100% safe and effective. The company simply covered up the severe adverse events by kicking those participants out of the trial and/or suggesting without evidence that the deaths had nothing to do with the experiment.
Remember, the CDC announced a few weeks ago that it had finally study a potential association between the COVID shots and strokes. Well, it turns out the agency had the opportunity to study it already in 2020 before a single human being outside the trial was injected. “Patient no. 11621327” was more than a mere number. He was a human being found dead from a stroke in his apartment just three days after the second dose. Typically, with a novel product in trial, any death – even one not so sudden – makes the product suspect until it is proven innocent. Yet in this case, Pfizer simply dismissed the death as not related to the vaccine, just as the company did with Patient #11521497, who died 20 days later from cardiac arrest.
The article also provides more details on the Buenos Aires trial site, the largest one in the world, in which attorney Augusto Roux was severely injured with pericarditis and liver damage. Instead of being recorded as a severe adverse event, he was marked as having had COVID (even though he tested negative) and was summarily removed from the trial. Roux was on my podcast last July and told me Pfizer refused to help treat his injury because officials felt it had nothing to do with the vaccine, and insurance also refused to pay for treatment because the insurance company blamed it on him willingly joining the trial.
Die Welt reports that on Aug. 31, 2020, 53 of those in the trial in Buenos Aires were unblinded and removed from the trial against the protocol, which calls for this only “in emergencies” (unless this was indeed an emergency!). By the end of the second dose, a further 200 individuals were removed from the trial, meaning that overall, more than 250 of the original 1231 participants were terminated, thereby making the entirety of the data from the largest trial site irrelevant to use in the final trial results.
Overall, 21 participants in Pfizer’s phase 3 trial died, as compared to 17 in the control group before they were unblinded, which should have been a red flag before the shot ever took off. Pfizer claimed there was no evidence anyone died from the vaccine, but after it’s been revealed that a number of people in the trial suffered heart ailments and strokes, the company’s defense holds no water. Yet here we are, over two years later, and the shots are still on the market, promoted like manna from heaven, and even mandated in most hospitals and universities, including in red states. How is this not the top public policy issue of our day?
Consider the following from a public policy standpoint. Pfizer gets the government to pony up billions in taxpayer dollars for the shots, several billion more to promote, advertise, distribute, and mandate them on every human being alive – all while absolving Pfizer of liability. So how do we know the shots are safe? Who gets to monitor the clinical trial? The very manufacturer that was absolved of liability by the government! The Die Welt article even mentions that Pfizer pushed through a liability waiver on its contract not just for negligence, but also for “fraud or bad faith on the part of Pfizer itself.”
Pfizer responded to the Die Welt reporter by asserting that, “Regulatory authorities around the world have approved our Covid-19 vaccine. These approvals are based on a robust and independent assessment of the scientific data on quality, safety, and efficacy, including the phase 3 clinical trial.” Sure, authorities guaranteed the company endless funding, marketing, mandates, and indemnity so that Pfizer would have no incentive to even release the true results of its trial, much less make the product better.
How can this continue to go on after all we know?
Yet in all honesty, this year’s legislative sessions in red states have been an utter disgrace – with medical freedom not even being on the back burner of policy issues. The few brave legislators who seek to impose some sort of accountability on the state departments of health for promoting and mandating these shots are summarily shouted down. Florida is the only state where officials are holding Pfizer accountable with the convening of a grand jury. Just last week, the Florida Department of Health sent an alert to doctors warning them to inform anyone inquiring about the COVID shots about the adverse events reported to the CDC’s VAERS. Where are the other red states? Why is Ron DeSantis the only governor who values the Nuremberg Code?
What is it going to take to give this issue the prominence it deserves so that the policies and laws reflect the human toll these odious policies have taken on humanity? How many more people need to die for a lie? Remember, a study from Thailand showed that 29% of young males in the study sample suffered some form of subclinical heart damage whether they experienced symptoms or not. We have potentially hundreds of millions of people in the world who are ticking time bombs and in need of the best research, diagnostics, and treatment.
Amid all the existential threats to our security, civilization, culture, and economy – and there are certainly many – can you think of anything that matches the severity of this issue? From died suddenly to plummeting birth rates, how is the vaccine issue not the top concern of all public policy, given that it was injected in 5.5 billion people and officials are on the cusp of approving more mRNAs? So we’re now supposed to believe Moderna’s own published phase 3 trial results of its RSV shot that it’s 84% effective and absolutely no serious adverse events occurred? Within months, if we don’t stop it, this shot will be in the arms of every senior and then, eventually, in the arms of every newborn baby.
After Pfizer purposely fabricated its clinical trial, the company must now be on the hook for a different sort of trial – one Steve Deace and I lay out in “Rise of the Fourth Reich.” Unless we begin holding pharma companies accountable and erecting legal firewalls to protect the people from their endless experimentation, they will do this again and again.
Imagine not only having injected 5.5 billion people with multiple doses of the failed COVID shots, but destroying lives and denying humane treatment on account of them. Now imagine knowing everything we know about the efficacy and safety of these novel therapies and still forging ahead with more doses and now RSV and flu shots built upon the same platform. Bad enough, right? Well, it gets even worse. Fauci now concedes that all respiratory viral vaccines are garbage, including those for flu, coronavirus, and RSV. Yet the policies never match the new admissions, as they race to accelerate the new flu and RSV shots within months.
In probably the most impactful story ignored by the media in recent weeks, Fauci co-authored an academic paper in Cell last month, along with the senior scientific adviser of NIAID, absolutely dumping on not just coronavirus vaccines, but all respiratory vaccines. It was a paper that could have been written by censored doctors like Ryan Cole, Peter McCullough, and Pierre Kory, and it reveals that Fauci indeed had a deep knowledge all along of the shortcomings of suboptimal antibody responses generated by this genre of vaccine.
First, the authors concede that flu vaccines are often only 14% effective and have never improved over the years. “After more than 60 years of experience with influenza vaccines, very little improvement in vaccine prevention of infection has been noted.”
Then they go on to admit that the vaunted COVID shots are in the same boat. “Deficiencies in these vaccines reminiscent of influenza vaccines have become apparent. The vaccines for these two very different viruses have common characteristics: they elicit incomplete and short-lived protection.”
Remember, to this very day, we still have children being kicked out of day-cares, people being denied organ transplants, and hospital workers losing their jobs on account of a premise that Fauci quite blatantly admits was false all along.
Fauci and company demonstrate the common thread between the failures of coronavirus, flu, and RSV vaccines in that respiratory viruses do not lend themselves to a blood-based antibody response, as so many of the doctors on my podcast have been saying for two years.
In stark contrast, the non-systemic respiratory viruses such as influenza viruses, SARS-CoV-2, and RSV tend to have significantly shorter incubation periods and rapid courses of viral replication. They replicate predominantly in local mucosal tissue, without causing viremia, and do not significantly encounter the systemic immune system or the full force of adaptive immune responses, which take at least 5–7 days to mature, usually well after the peak of viral replication and onward transmission to others. … As a result, the non-systemically replicating respiratory viruses, apparently including SARS-CoV-2, tend to repeatedly re-infect people over their lifetimes without ever eliciting complete and durable protection.
Fauci et al. ask the question: “If natural mucosal respiratory virus infections do not elicit complete and long-term protective immunity against reinfection, how can we expect vaccines, especially systemically administered non-replicating vaccines, to do so?”
Say what?!!! This got me banned from Twitter for six months! Fauci is acknowledging that this genre of vaccine – before we even explore the dangers with spike protein, mRNA, and lipid nano particles – simply does not target the virus in the respiratory tract and in fact never achieves immunity! You can keep getting the virus again and again, as we now see. But nothing that he is positing is new. This is not some new revelation. From reading the piece, it’s clear Fauci understood this principle of immunology all along. Yet to this day, there are still COVID shot (and even flu shot) mandates looming over the military, medical settings, schools, and other important places.
It’s not just a lack of efficacy on transmission. As we’ve been warning for two years based on doctors who got this right from day one, whenever you have a leaky, waning vaccine built upon suboptimal antibodies with a rapidly mutating virus, it creates immune tolerance and imprinting so that the misfiring of the immune response actually generates negative efficacy. While this paper does not officially acknowledge negative efficacy, it does acknowledge the concern of “disease tolerance” and “immune tolerance,” which stem from “immune defense mechanisms that allow hosts to ‘accept’ infection and other antigenic stimuli to optimize survival.”
Given that we now see endless negative efficacy associated with the COVID shots and numerous studies showing a misfiring of antibody classes, why is there no concern that this shot and other respiratory viral shots are causing immune tolerance leading to negative efficacy? Numerous flu shot studies warn about the shots tamping down T cell responses and making people more vulnerable to infection. Moderna’s clinical trial of COVID shots for babies seemed to be associated with a dramatic increase in RSV cases, which seemed to play out globally during the off-season surge of RSV in the summer of 2021 and the early fall of 2022.
So this is not just about failure to stop transmission, but also about clinical outcomes as well as negative efficacy. A Canadian study of vaccine efficacy during the 2018-2019 flu season found negative efficacy for some age groups because “vaccine mismatch [a form of original antigenic sin] may have negatively interacted with imprinted immunity.”
Despite all the fanfare around the flu shot, a 2005 study published in JAMA soberingly found that there was no correlation between “increasing vaccination coverage after 1980 with declining mortality rates in any age group.” The only mortality decline researchers discovered was against H3N2 in those born before the 1968 pandemic because of natural immunity, not the vaccines.
Despite everything we now know (and people like Fauci clearly knew for years), you can’t go into a pharmacy for half the year without being harassed to get a flu shot, and many schools and places of work strongly encourage if not mandate it. But do any of these fake medical practitioners even understand the issues with suboptimal antibodies, negative efficacy of the flu shots, and immune suppression of T cells?
Fauci and company conclude the paper with a shocking concession about these long-standing respiratory vaccines and the ones currently being studied, including RSV vaccines:
Challenges to developing next-generation respiratory vaccines are many and complex (Table 2). We must better understand why multiple sequential mucosal infections with the same circulating respiratory viruses, spread out over decades of life, fail to elicit natural protective immunity, especially with viruses that lack significant antigenic drift (e.g., RSV and parainfluenzaviruses), if we are to rationally develop vaccines that prevent them. We must think outside the box to make next-generation vaccines that elicit immune protection against viruses that survive in human populations because of their ability to remain significantly outside of the full protective reach of human innate and adaptive immunity.
Any sane person reading these statements does not get the impression that Fauci believes we are just weeks away from cracking the code on RSV shots. He believes the challenges are “many and complex,” are prone to mutation with “antigenic drift,” and require “outside the box” thinking to “make next-generation vaccines.”
With remarks like this from the undisputed champion of the vaccine movement, how are we to accept an RSV and flu shot – not just on the traditional platform but on the dangerous mRNA platform – being forced upon us within months through expedited review? How do we not have legal safeguards in place to subject Moderna, essentially created and funded originally by DARPA, to liability and to prevent all mandates, coercion, and pressure to take it? How do we not have a better pharmacovigilance system in place? How do we not fix what went wrong with the trials for COVID? Then again, the FDA plans to keep producing and administering the same COVID shots that are for variants that don’t exist, which Fauci acknowledges in this piece is a function of the problematic antigenic drift.
Do facts no longer matter? Do human lives no longer matter? And for what? For the flu and RSV that we’ve lived with for decades?
Despite everything we are seeing about respiratory viral vaccines failing and mRNA not staying in the shoulder muscle, the FDA has granted Moderna “breakthrough therapy” designation for its RSV mRNA shot. This is a status usually granted for targeted treatment for deadly ailments that allows the FDA to speed up approval process, yet it is now being used for a virus that’s been around for decades and with a biological platform that everyone agrees has just failed. Pfizer and GSK also have RSV shots in the pipeline, and both Moderna and Pfizer have mRNA flu shots likely to be released later this year.It’s quite evident at this point that all of the safety nets protecting the public from Joseph Mengele-like experimentation have been breached. Our will to fight back is all we have left.
Like Blaze News? Get the news that matters most delivered directly to your inbox. SIGN UP
With the exception of the COVID shots, there is perhaps nothing in the economy that has gotten more tailwind in terms of government support than electric vehicles. Whether it’s the subsidies, the mandates, the inflation of the cost of gasoline, or the construction of cumbersome electric charging infrastructure, the government has done everything it can to turn a product that is inherently costly and impractical into something accessible to the public. Yet despite it all, a new study shows fueling these cars is more expensive than most gas-powered cars, even with record high gasoline prices, which were induced by policies from the same green energy. Now is the time to end all subsidies and mandates on behalf of this pathetic industry.
It’s truly hard to quantify the degree to which government has propped up green energy and products that never would have gotten off the ground in the free market. Between making gasoline so expensive and making gas cars more expensive with fuel efficiency mandates on the one hand and subsidizing electric vehicles and all their required infrastructure on the other hand, electric cars have every reason to succeed. Heck, all blue states are even signaling the end of gas-powered cars altogether, and some are even mandating it. The subsidies reached a tipping point with the “Inflation Reduction Act,” which offers a subsidy of $7,500 per electric vehicle. But a new study shows that it still costs more to fuel an EV after spending so much more for the original purchase.
“Typical mid-priced ICE car drivers paid about $11.29 to fuel their vehicles for 100 miles of driving,” concluded a study from consulting firm Anderson Economic Group. “That cost was around $0.31 cheaper than the amount paid by mid-priced EV drivers charging mostly at home, and over $3 less than the cost borne by comparable EV drivers charging commercially.”
Oh, and let’s not forget that time is money. You have to spend an average of $18 per charge and spend 15 minutes per 100 miles traveled. Good luck on your family road trip this summer with the baby screaming in the car who was woken up after finally taking a nap, thanks to the incessant need to stop.
The only benefit the Michigan-based consulting firm found to fueling EVs over traditional cars was, of course, among the high-end luxury cars used by the elites promoting these products.
This is astounding given the record-high gas prices this past year, especially for winter months. This means that even after spending more money for the purchase of an EV, you are saddling yourself with a boondoggle to maintain. The problem for the parasitic, venture socialist industry is that the very regressive green policies that are harming the oil and car industries are doing even more damage to the electric grid. Thanks to the war on coal, oil refineries, and pipelines and the stagnation of nuclear energy by the same radical eco groups, electricity prices are skyrocketing even more than gasoline. All that “investment” in solar and wind is not there for us during our time of need. Now we face the prospect of electric grid failures more acutely than even oil and gas shortages.
Just consider what would happen during these heat waves if we only had electric vehicles. California grid operators warned people during last summer’s heat wave to ease off charging their cars. Now imagine if they had their way and 100% of cars were electric and 100% of the electricity was generated from wind and solar. Well, you’d be stuck at home … which is exactly how they want it.
Biden’s signature legislation last year handed out over $50 billion to the electric vehicle industry, including $7.7 billion for EV charging stations and $10.3 billion in grid and battery subsidies. But just like money can’t buy you love, it also can’t buy you efficacy, efficiency, or safety. Despite all of the corporate welfare for green energy, it’s still natural fuels from the earth that are holding up Texas’s grid during this cold spell and ice storm in the northern part of the state.
Texas Grid Snapshot… yet 8 out of 10 new projects are wind and solar
What was powering northern Texas during the ice storm? As the Energy Information Administration data shows, natural gas was the star player while wind collapsed, despite Texas throwing tens of billions of dollars at it.
As for efficiency, a 2021 study shows that even if EVs were more economical post-purchase in terms of fueling per mile, there are fewer miles to monetize those returns. According to the paper from the Bureau of Economic Research, the average family EV only racked up 5,300 miles per year, less than half the 13,476 miles per year driven by normal privately owned cars. Thus, the savings in operating these cars was always a mirage because they are just driven less. They could never possibly replace internal combustion vehicles, just like wind and solar cannot replace oil, gas, and coal for electricity and fuel. Yet the government has mandated automobile manufacturers to quadruple the market share of EVs in their fleets.
Then, of course, there is the issue of safety. Recently, it was found that during Hurricane Ian, electric vehicles caught in the storm surge in southwest Florida were suddenly exploding. DeWalt’s new no-turn electric mower also seems to have problems, as one model caught fire on the opening day of Equip Expo 2022. These are the sorts of issues that are worked out when a product has to rise or fall in the free market without a permanent guarantee of income. But with endless subsidies, we can only imagine the economic and societal problems from an EV-only road show.
Moreover, what this all demonstrates is that EVs were never meant to replace traditional cars to fulfill our needs and standard of living. They are serving as a Trojan horse to break our standard of living so that we will “own nothing and be happy,” as the WEF officials like to say. They want us to pay a fortune for cars and then barely be able to drive them because of the cost of electricity that they are concomitantly and artificially increasing thanks to other global warming regulations and market distortions.
Oh, and of course, no action taken against our prosperity, liberty, and mobility is complete unless it helps China. We all know China controls 76% of global EV battery production, and the nickel, cobalt, and lithium used to produce these batteries are all produced abroad. So now we are subsidizing China and other bad actors to make the rope that hangs our economy, which is pretty much in line with every other government policy. All they need now is to absolve these companies of product liability, and they will be just like the COVID shots. So why do Republican governors continue to service the electric vehicle scam? Why do they continue to place the boot of government on the scale toward these loser vehicles? The time has come for red states to completely divest from the green energy scam.
“During the course of the experiment the scientist in charge must be prepared to terminate the experiment at any stage, if he has probable cause to believe, in the exercise of the good faith, superior skill, and careful judgment required of him, that a continuation of the experiment is likely to result in injury, disability, or death to the experimental subject.” ~Nuremberg Code #10
We’ve reached a critical mass of data points and safety signals on the COVID shots from a full two years of it circulating in 5.5 billion people. One must be worse than a conspiracy theorist to ignore them. One now has to be a “coincidence theorist” to chalk up this degree of human suffering that is in immediate need of redress to mere coincidence.
It’s time for Republicans in state legislatures and on the House Select Subcommittee on the Coronavirus Pandemic to pay attention to the daily barrage of shocking data points and safety signals. Here is just a sampling of 12 points from the past few weeks, out of many more. Each one alone should have been enough to suspend the shots, terminate the technology in the pipeline, and investigate the actors behind it. Time is of the essence:
1) 17% of children experienced some cardiac symptom after the Pfizer shot: Just how large is the universe of those roped into some risk of cardiac damage? A new peer-reviewed study from Taiwan published in the European Journal of Pediatrics found that 17% of high school children, mainly boys, experienced at least heart palpitations or chest pain from the second dose of Pfizer. These numbers work perfectly with many other surveys showing a significant number of people experiencing arrythmias, tightness in the chest, or shortness of breath. They are also particularly concerning given that a Swiss study and a Thai study showed the proportion of people afflicted with subclinical myocarditis (a ticking time bomb) was much larger than those diagnosed with myocarditis.
2) 20% spike in excess deaths in England and Wales:According to the latest figures from the U.K.’s Office for National Statistics, deaths for the final two weeks of 2022 in England and Wales were 20% above the five-year average. That is greater than the pandemic itself. It makes no sense why there would be more deaths, long after the vaccines supposedly quelled COVID, than in 2020 and early 2021, at the peak of the pandemic. The U.K. Timesreports that “50,000 more people died last year than normal.” That is the equivalent of 250,000 excess deaths in the U.S. This cannot be COVID; it must be something else. (The data for those weeks: Data from week ending Dec 23, 2022; data from week ending Dec 30, 2022).
3) 0 of 1,1779 COVID hospitalizations in New South Wales were unvaccinated:According to NSW Health, which breaks down COVID hospitalizations and deaths by cohorts of various levels of vaccination, for the two weeks ending Dec. 31, 2022, not a single COVID hospitalization (or ICU admission) was among the fully unvaccinated.
The overwhelming majority were among the boosted. Although 84% of people in Australia have gotten at least one dose of the shot, it’s not 100%, so there is clearly a degree of negative efficacy, which is in itself a safety signal. And although 6% of the deaths were among the unvaccinated (still below their share of the population), it is suspicious how they all seemed to die at home, which makes you wonder if they are placing some of the “unknown” category into the unvaxxed pile by automatically assuming they didn’t get the shots. Dr. Syed has presented evidence in the past that makes it likely NSW Health has been doing that all along.
4) FDA admits massive elevated risk for heart attacks, blood clots, and pulmonary emboli: FDA researchers published the results of a massive observational study of 30.7 million Medicare patients in 2021 and found that people who took the shot found that the shots increase risk of pulmonary embolism by 54%, acute myocardial infarction by 42%, blood clotting by 91%, and platelet disorder by 44%. The claim this is only an early warning signal and downplay the results, but they harmonize with many other surveys, studies, reporting, and an understanding of the shot’s mechanism of action.
5) COVID vax was associated with 22%-74% greater all-cause mortality vs. being unvaccinated in U.K.: Prior to May 2022, the U.K. Health Security Agency published COVID case and death rates, age-stratified, by vaccination status. They terminated these weekly reports after we began using them against the system. El Gato Malo revisited the numbers and calculated somewhere between a 22% and 74% elevated risk of all-cause mortality associated with the vaccinated from September 2021 through April 2022.
As you can see, this portends either negative efficacy or risk outweighing reward even for seniors over 80 who are constantly bombarded with endless boosters. This should not come as a surprise given that Pfizer’s own all-cause mortality analysis in its six-month follow-up of its trial published in the New England Journal of Medicine showed 21 deaths in the trial group and 17 in the placebo group. The company failed to follow through the rest of 2021 and 2022, but it’s reasonable to presume based on what we know now that the negative efficacy became worse with other variants. It’s also likely that the long-term injuries of the vaccine, which were never followed because of the unblinding of trial participants, came home to roost increasingly over time.
6) New bivalent booster even worse: Remember the boosters that were approved with nothing but antibody tests and 8 blind mice? Well, now there are results of clinical trials for the bivalent booster approved last September, and members of the FDA advisory committee are expressing anger at not seeing this data. It turns out that 1.9% of the study participants who received the original booster became infected, while 3.2% of those with the new bivalent shot got COVID. This in itself demonstrates that not only does the detection of more antibodies not necessarily mean better clinical outcomes, but more antibodies of the wrong type can facilitate infection.
7) Two studies show mRNA shots create wrong antibody class: In yet another possible indication that the shots actually make you more vulnerable to coronavirus, a second study has been published showing the shots create a class switch from IgG1-3 neutralizing antibodies to IgG4 “tolerating” antibodies, which can make someone keep getting the virus and not fight it off. Last month, German researchers, in a groundbreaking study published in Science Immunology, found that some people reinfected with the virus after having had boosters had over 40% of their antibodies composed of IgG4. Now a second peer-reviewed German paper, this time published in Frontiers in Immunology, found this phenomenon even after the original two doses. The shocking thing is that a Pfizer scientist served as the study’s editor and one of Fauci’s staffers at the National Institute of Allergy and Infectious Diseases served as a peer reviewer
8) New bivalent shot caused reactions in large minority of children: Not only do the boosters not work, but according to the CDC’s own V-SAFE adverse reporting app, 49% of the 5- to 11-year-old children who took the bivalent booster shot experienced systemic reactions. These symptoms include fatigue, chills, nausea, abdominal pain, vomiting, joint pain, and diarrhea. In 22% of the children, they could not go to school or perform their daily functions after getting the shot. In other words, these children experienced upfront the upper bounds of what the virus would have done to them. And keep in mind that V-SAFE did not monitor lurking serious long-term side effects – all for a shot that doesn’t work.
9) 51% of Democrats believe vaccines behind sudden deaths: Whether the government and media are willing to acknowledge the extent of injuries, the dam is clearly breaking with the general public. Numerous surveys have been showing for months that most people know friends or family killed by the shots. But earlier this month, Rasmussen published a survey broken down by party affiliation. It found that 51% of Democrats nationally believe it is likely the vaccines have caused a significant number of unexplained deaths, and 33% believe someone they know personally died from the shot. That is more than the 26% of Republicans and Independents who said the same thing. The reason this is significant is because more Democrats than Republicans received the shot, so these results likely reflect reality.
Furthermore, 31% of Democrats attest to experiencing side effects, and 6% believe they experienced major side effects. This tracks closely with the 7.7% according to the CDC’s V-SAFE who had to seek medical attention (and 33% experienced at least minor side effects). And this is among Democrats who are naturally inclined to defend the shots, which means this is not some right-wing conspiracy but a reflection of widespread reality.
10) VAERS analysis shows 500 injuries with greater safety signals than myocarditis: By now, anyone not under a rock knows that the vaccines could cause myocarditis. But according to a FOIA document obtained by the Epoch Times, in turns out that the CDC conducted its own analysis of VAERS from December 2020 through July 2022 and found that there were over 500 categories of injuries with louder safety signals than even myocarditis. Specifically, as Hebrew University Professor Josh Guetzkow explains, there are 503 AEs with proportional reporting ratios larger than myocarditis and 552 with PRRs larger than pericarditis. Overall, in just a year and a half of Moderna’s and Pfizer’s COVID jabs, the safety signals were 5.5 times larger than all serious reports for vaccines given to adults in the US since 2009.
11) The CDC anticipated over 1,000 VAERS reports per day: The agency didn’t make a mistake. Bureaucrats knew from August 2020 that they expected major problems with the vaccine. Prof. Guetzkow, the prolific FOIA sleuth, posted details of documents showing that the CDC contracted with General Dynamics in August 2020 to run the VAERS database. The $9.45 million contract stated that officials expected 1,000 adverse event reports a day, with 40% of them being serious. Again in March 2021, they amended the contract to expand the capacity by another 25,000 a day and to clear a backlog of 115,000 reports just for the first ten or so weeks of the vaccination drive.
12) Disability numbers skyrocket in U.S. and U.K. coinciding perfectly with vaccine take-up: The U.K.’s Institute for Fiscal Studies published a report last month showing that the number of people on disability claims doubled in the U.K. from the summer of 2021 to July 2022.
While this alone doesn’t prove causation, in conjunction with the millions of reported debilitating injuries, the timing of this rise makes the shots the number-one suspect relative to any other possible factor. It is possible that lockdowns are a part of the problem, because the disabilities were heavily weighted toward mental health problems among younger people. However, the doubling of claims across all age groups, with physical ailments being the key cause among the middle-aged, makes it hard to pin this trend exclusively on lockdowns. They also note that this trend of doubling of disability payments “is consistent with the rise being driven by a general worsening of health across the population,” which in itself coincides perfectly with the “significant rise in the number of (non-COVID) working-age deaths from late 2021 through 2022, compared to pre-pandemic years.”
It should be noted that a similar trend is evident in the United States. According to the Bureau of Labor Statistics, those in the labor force identifying as having a disability skyrocketed by more than 30% right after the vaccines were introduced to the public. This is unprecedented and did not begin in 2020 with COVID and the lockdowns.
The goal of the CDC and FDA at this point is to create a limited hangout in which they let the pressure mounting against the shots out of the balloon and channel it into a limited concession. For example, the CDC conceded some sort of safety signal for myocarditis, then briefly conceded a safety signal for strokes in seniors on the Friday afternoon headed into the MLK holiday weekend before concluding in a comprehensive study that took all of a few hours that it’s really not a problem.
In reality, there are over 14,000 categories of injuries reported to VAERS affecting every organ system and every inch of the body. If you just take the 1,400+ SERIOUS adverse events noted by Pfizer in its confidential document just 90 days into the vaccination campaign, it would take 10 minutes (reading at the rapid rate of 200 words per minute) to disclose them in a TV commercial. Yet Pfizer is exempt from such disclosures.
Consider the fact that in 1999, Dr. Fauci explained to Congress that you can have a vaccine that is totally fine at first, but then as late as 12 years later, “all hell breaks loose.”
The year is 1999. A virus (HIV) is killing people. Anthony Fauci warns:
"If you give people a vaccine & a year goes by…everybody's fine. Then you give it to thousands of people, & 12 yrs later all Hell Breaks Loose. Then what have you done?"
There is nobody alive at this point who could possibly ignore the dangers of the mRNA COVID shots. Rather than taking them off the market and immediately investigating who knew what and when, the same companies are now filing with the FDA to immediately introduce more mRNA shots into the market. They will immediately be championed by every county and state health department and promoted by every pediatrician until they’re in the arms of every newborn baby. The mRNA flu and RSV shots are just around the corner, and if states do not place legal barriers to their release, they could possibly do even more damage than the COVID shots, if that is even possible.
Moderna is so brazen and shameless that even as millions are suffering from their first mRNA shot, the company is announcing that its new RSV mRNA shots are … you guessed it … 84% effective. Well, judging by the COVID shot that they said was 94% effective from day one but in fact is now suffering from a bout with negative efficacy, we can only imagine how “safe and effective” a jab that is advertised as “only” 84% effective might be. Pfizer’s Albert Bourla also announced the company will have an mRNA flu shot out in June or July and then another combo coronavirus/flu shot based on an mRNA platform sometime later in the year.
After Moderna leaked the top-line results of its own in-house study (no third-party studies needed, of course), Stephane Bancel, the company’s CEO, told CNBC at Davos that the company was able to complete all three phases of the RSV vaccine clinical trial in just one year (instead of six to eight years) and will now file for expedited approval with the FDA so that it’s on the market for this coming fall. A nice follow-up to his revelation that the company already worked on the COVID vaccine before the virus had a name!
Moderna CEO Explains How Their Vaccine Has Your Cells Produce a "Key Protein of the RSV Virus"
"We started the Phase 1 for the RSV vaccine in Jan 2021. And we are just 24 months after announcing Phase 3 positive data. So think about how we have [reduced that] from 6-8 years." pic.twitter.com/SCpn1a4Yov
Consider the fact that RSV was the poster child for a failed vaccine in the 1960s and the pharmaceutical industry has been unable to produce an effective shot for 55 years. Yet we are to believe that the company was somehow able to magically crack the code, and of course, it won’t replicate any of the problems the COVID shot induced. Has anyone ever wondered how a company that failed to bring a single product to market for eight years could abruptly become the star player in the biggest pandemic ever and then suddenly have more than a dozen mRNA products ready to go?
Well, after we solve the question of how Moderna seemed to have patented the sequence for the COVID virus in a cancer drug the company was developing in 2016, perhaps we can discover the secret to its success.
Maria Bartiromo: 'Why is Moderna's patented sequence in the Wuhan coronavirus?' Moderna CEO Stéphane Bancel: 'We're looking into it.' Maria: 'OK. Thx for all your help!'
Incidentally, 11 months after Maria Bartiromo asked Bancel about Moderna having patented the sequence, he still has not gotten back to us about the reason behind the great coincidence. What we do know is that a company that seems to ascertain the future more than a Biblical prophet is now asserting that there will be more pandemics and is making it clear it now has mRNA production in every continent.
DAVOS WATCH: Stéphane Bancel, CEO of Moderna says “the pandemic is still ongoing” and “we all know” there will be other outbreaks and pandemics
He also lays out his plan to build more MRNA Vaccine factories on every continent across the globe #wef23pic.twitter.com/IuqiXpcw3T
Even before discussing the RNA platform, we must realize that RSV is the worst candidate even for a traditional vaccine. One of the things we should all have observed from the COVID shots is that rapidly evolving RNA viruses are prone to mutation, and the antibody responses stimulated by shots don’t seem to be a good match for respiratory viruses. This is why even the CDC admits the flu shot was only 16% effective last year, which makes us wonder if the real number is in negative territory. Suboptimal antibodies or a mismatch of classes of antibodies can create immune imprinting and allow the body to either tolerate the virus more or serve as a Trojan horse to enhance the virus, which is what happened with the old failed RSV shot.
The RSV vaccine of 1967 was an utter disaster, resulting in the hospitalization of 80% of the infants and toddlers in the clinical trial. Children’s Hospital of Philadelphia, on its website, explains that the RSV shot was a textbook example of misfiring antibodies creating antibody-dependent disease enhancement, whereby the “antibodies act as a ‘Trojan horse,’ allowing the pathogen to get into cells and exacerbate the immune response.”
“In clinical trials, children who were given the vaccine were more likely to develop or die from pneumonia after infection with RSV,” states the website of the prominent children’s hospital. “As a result of this finding, the vaccine trials stopped, and the vaccine was never submitted for approval or released to the public.”
Now let’s get to the mRNA platform. While it’s true that many of the problems with the COVID shots stem from the spike protein, which is why every version of the shot out on the market is problematic, the mRNA itself is also dangerous. What should be self-evident to anyone at this point based on literature that was published pretty early on is that there is no shutoff or modulator of the mRNA coding your body. So even if it doesn’t code your body to produce something as harmful as a pathogenic spike, there is no ability to ensure the mRNA doesn’t go throughout your entire body producing that protein, tissue, or code for an unlimited period of time and in unknown quantities. Almost nothing is purely good in unlimited quantities and unlimited locations in your body for an unlimited period of time.
This is before we even focus on questions of the pro-inflammatory nature of the lipid nano particles delivering the mRNA, the polyethylene glycolcasing around it causing autoimmune and allergic reactions, and numerous other materials that have never been properly studied. Then of course there are a number of studies that indicate a substantial risk of the mRNA reverse transcribing into DNA:
Shouldn’t we conclusively rule out the concerns of DNA transcription raised in these papers before truncating the next mRNA development from eight years to one year?
Thus, aside from targeted therapies for terminally ill patients, clearly mRNA is not ready for prime time and must be banned, because clearly the system will not self-regulate. Vaccination has become a cult with no qualification, circumspection, modulation, or balanced rational thought. As Mike Ryan, an Irish doctor who serves as executive director of the World Health Organization’s Health Emergencies Programme, recently said, “Vaccination is about protecting yourself, but it’s also an inherently altruistic act — you’re vaccinating yourself in order to be part of an immune group that will then protect those who can’t be vaccinated.” It’s therefore quite obvious they will target the RSV shots to children with even more cultish devotion than the COVID shots.
Everyone knows that babies are more vulnerable to RSV and the flu than to COVID. The companies will engage in full-court press to get this shot in the arms of every baby. Blocking mandates is not good enough. We have more than enough information to demonstrate that these shots are dangerous and are not ready for prime time. Every state must ban its own health department from purchasing, promoting, recommending, or marketing these shots. Furthermore, every state needs a commission of diverse voices to shadowbox the FDA and make its own recommendations, similar to what Governor Ron DeSantis established under the guidance of Dr. Joe Ladapo.
Most Republicans are willing to fight intrepidly against abortion, even when it’s politically unpopular. Yet mRNA shots are like a forced abortion because the minute they are permitted, even if they are not mandated, there is no enlightened consent. Unsuspecting parents, pregnant women, and seniors will be pressured into getting them. We still don’t know the extent to which they might shed on other people. Also, there is a robust effort from a $26 billion industry to inject them into the beef supply.
Most of all, while states create a backstop against federal-pharma experimentation, it’s incumbent upon Republicans in the House to repeal pharma’s legal immunity to liability. That is the best way to ensure that vaccines are safe and we can discover any malfeasance in court. Absent these reforms, they will continue to experiment upon our children. And what do they care if countless lives are lost or injured? They’ll just produce the mRNA to “fix it,” like they are planning with their much-anticipated mRNA cure for heart attacks!
Medical freedom needs to become the new pro-life movement on the right. It quite literally affects even more human beings than abortion.
This week, all eyes in the political world will turn to Washington as the excitement builds over the transition of power in the House of Representatives. But what good is a narrow RINO majority in just one branch of the federal government when Republicans ceded the budget leverage they otherwise would have commanded this month? Why not focus on half the state governments where Republicans enjoy trifecta control, in most of them with supermajorities in the legislatures? Indeed, this year kicks off the most important legislative sessions of our lifetime. The intensity of grassroots pressure placed on these equivocating Republicans will determine whether red-state America is just a pro-gun, anti-abortion version of blue-state hell or whether we can fully reconstitute the America we once loved in portions of the country.
There’s no reason to focus on the presidential election and what might happen two years from now. We can’t wait two years for change, nor are we likely to actualize it on the federal level. The American Revolution was catalyzed by state legislatures organizing together. The reconstitution of that revolution will also have to unfold in the bodies of government closest to the people, at least in the states where a majority of the people haven’t already succumbed to the spirit of the age.
Throughout the next few weeks, I’ll be posting legislative goals for various issues, but for today, we will focus on the most important issue of our time: medical freedom. It is the ultimate pro-life issue of our time. There is no evidence that the genocide that has occurred over the past few years from COVID and COVID fascism is even being addressed at the federal level. Therefore, it is up to the red states to reconstitute the Nuremberg Code and learn the lessons from the travesty of Covidstan.
Here are the legislative ideas and objectives that must be pursued in red states this session. If not now, while the malfeasance of the government is fresh on the minds of the people, then it will never be accomplished. This is a checklist of ideas that activists should use to determine whether there is legislation in your respective states addressing the issue of our time – to ensure there are legal, structural, and political barriers in place so that what occurred the past few years is immediately halted and cannot happen again.
Permanently ban all COVID biomedical security mandates:
Now is precisely the time not only to reverse the COVID policies, but to plow over the ground of tyranny and salt it with provisions permanently banning and even criminalizing its implementation. This means banning all public and “private” mask and vaccine mandates in any setting under any circumstance. This is no longer 2020 when we were merely playing defense. Now we have reams of data and studies showing these policies are not only ineffective but downright harmful.
Until now, some states agreed to a health care exemption from the prohibition on mandates, but that is precisely the setting where cancer patients, pain patients, and Alzheimer’s patients who are forced to use medical services regularly are still being coerced to cover their faces. This is unacceptable. Disability law mandates affirmative accommodations for people with health issues, yet somehow we are to believe hospitals can force patients to wear something hazardous? The bill must be backed by a stiff fine for any violator, and in the case of anyone caught forcing schoolchildren to wear a mask, there must be prison time.
Make health status a protected class under anti-discrimination law:
One way of accomplishing the aforementioned goal is to codify health status into state anti-discrimination law, making it unlawful to discriminate in any way on account of opting against a particular medical intervention to one’s body. It might also be worthwhile codifying such rights into the state’s constitution along the lines of the following: “The right of a person to refuse any medical procedure, treatment, injection, device, vaccine, or prophylactic shall not be questioned or interfered with in any manner. Equality of rights under the law or in the realm of public accommodation shall not be denied or abridged to any person in this State because of the exercise of the right under this section.”
Preserving doctor-patient autonomy:
No doctor shall be penalized with loss of licensure or board certification on account of speaking out against vaccines and mask-wearing.
No doctor can be punished for using off-label FDA-approved drugs, and all pharmacists must fill such prescriptions absent a religious conscience concern. There should be a cause of action in court for patients to sue pharmacies that block valid prescriptions.
Also, any barriers to doctors themselves dispensing drugs they prescribe should be lifted. Some states allow doctors to dispense drugs in the office, but this power is generally limited and must be expanded.
Finally, the complaint process against doctors with the state’s medical board must be overhauled. Complaints can only be accepted from patients alleging injury, surviving family of injured patients who die, or from medical professionals with direct contact who allege patient harm. All complaints in absence of patient harm must be ignored.
Abolish the state’s immunization register:
No good will come of the state holding onto a person’s vaccination status, and it will only be used to enforce the biomedical security state and should therefore be abolished. At a minimum, anyone administering a vaccine must obtain written consent from the patient prior to reporting the administration of a vaccine or immunization to the statewide immunization registry.
An immediate termination of mRNA vaccine promotion:
We are long past the time when the shots should merely not be mandated. The jabs must be taken off the market. State legislatures must bar their respective departments of health from promoting or purchasing any mRNA vaccines, ban all marketing or advertising of the COVID shots, create a commission to study the effects of the COVID shots by researching all those who died within 30 days of vaccination, and force the departments of health to fund treatment and diagnostics for those injured by the shots. Also, depending on state law, legislatures should follow Florida’s lead and work to convene grand juries to investigate the willful misconduct of hospitals, the departments of health, and the pharma companies throughout the pandemic.
Suspend the childhood immunization schedule:
All state indulgence and recognition of the CDC’s childhood vaccination schedule must be suspended pending the outcome of a commission to study the need, safety, and efficacy of every vaccine category and prototype on the market. Health departments could still support the other shots pending the commission’s recommendations, but all health care and school settings would be prohibited from discriminating against those who opt out of those shots.
Patient Bill of Rights for those in hospitals and senior care facilities:
Some states have pursued a few of these ideas, but there must be strong criminal and civil penalties for violators. Every hospital or senior care facility must always:
allow one surrogate present in the hospital (or as a visitor in a nursing home);
permit patients to access FDA-approved drugs off label prescribed by a doctor at their own expense if they agree to assume liability;
accord every patient the right to refuse any hospital-prescribed treatment or the right to refuse to remain in the facility if they have the mental capacity to leave (a ban on medical kidnapping).
There must be a cause of action created to sue any hospital and possibly for the district attorney to bring criminal charges against hospitals that deny these rights. All hospitals violating the patient bill of rights should be on the hook to lose state tax-exempt status.
A complete ban on remdesivir:
There is no sane doctor alive who can look you in the eye and declare remdesivir to be a safe and effective drug. Yet to this day, it remains the standard of care for inpatient COVID care. States must ban its use as they would any toxic and potentially lethal drug with zero benefit.
Ban on medical kidnapping via child protective services:
There is a growing trend of hospitals or doctors working with the state’s child protective custody agency to steal children from parents who refuse to go along with their course of treatment or bio-medical goals. States must ban all investigations and agency decisions to suspend parental rights on account of a parent’s refusal of specific medical treatments, diagnostics, or devices unless there is proof that the parent acted with malicious intent. Idaho House Bill 821 is a good model. This includes refusal to engage in masking or vaccination of a child. Also, such actions, opinions, or beliefs shall not be used as a factor in family court in determining custody arrangements.
Hold pharma accountable:
Although the federal government protects vaccine companies from liability, and this issue must be redressed at the federal level, states can still broaden their consumer protection and anti-fraud statutes to target pharma for blatant fraud. There is a wealth of material showing that the manufacturers knew the vaccines didn’t work and injured people, yet falsely marketed them. Also, state health departments, which assiduously pushed the vaccines in red states just as much as blue states, must use their remaining COVID funds to fund diagnostics, detection, and treatment of vaccine injury.
State legislatures should also form commissions to study the scope of injury through studies, death certificate and medical billing data, and investigating all deaths in the state within 30 days of taking the shots. Finally, they must create a state-based vaccine adverse events reporting system that is user-friendly and must use state resources to require and encourage medical professionals to report injuries to that system.
Ban endorsement of experimental shots:
States must bar their respective health departments from endorsing or marketing any shot to the broad public that has not undergone a human clinical trial with a sustained and maintained placebo control group. That clinical trial must have some third party supporting its safety data, which is independent from the manufacturer. Any trial based on “immonobridging” – measuring antibody titers and comparing them to various study groups – does not qualify.
Criminalize gain-of-function research:
There’s no need to wait for the feds to act. States should ban research institutions from engaging in gain-of-function research with a statute backed by criminal penalties. Individuals potentially harmed by such research should be granted a cause of action to sue those institutions.
Tax-credits for direct primary care:
Some states are already doing this, but there is a need to even the tax playing field between “cartel” health care and direct primary care. The core problem we experienced during the pandemic was a lack of individual thinking among practitioners, much of which is connected to the fact that they are all controlled by systems, insurance companies, and networks. With so much tendentious governmental treatment for the current cartel, states need to find ways to even up the score to incentivize people to use more free market and free-thinking doctors. Offering direct primary care the same tax benefits – both on the employer side and individual side of the ledger – we offer to the insurance companies is a good start. How many of these ideas have already been adopted by your governor? How many are represented by a piece of legislation pending in your legislative body? Now is the time to get to work. If not us, who? And if not now, when?
Tolerance is a good thing in most aspects of life. But when it comes to the immune system, artificially juicing up the body to create antibodies with long-term tolerance to a pathogen is a recipe for disaster. Amid thousands of papers on COVID and the vaccines, a new German paper published in Science Immunology should be the headline story this week. Although the subject matter is very dense, the implication of it is that the Pfizer shots (and possibly other mRNA spike protein shots) caused the immune system to misfire, thereby creating an endless feedback loop of viral immune escape, perpetuating the pandemic in the macro, and creating immune suppression for the individuals who received them.
The vexing question of 2022 is why the virus is even still with us to this day. Why is it that so many countries in the Pacific Rim that did so well in 2020 and 2021 now have a bigger problem in 2022 with less virulent strains of COVID? Why does it appear the pandemic will never end and so many people continue to get the virus multiple times? None of this is normal.
Wherever you turn, the most vaccinated countries are not only experiencing rampant side effects from the shots, but worse outcomes from COVID itself following their endless booster campaigns.
During the last six months, 98% of all reported covid deaths have occurred in nations where more than 1 vaccine dose has been administered per person.
Portugal is the most vaccinated nation in all of Europe (95% vax'd, 70% boosted) and yet just as many people are dying now as in 2021 and significantly more people than in 2020 (when no one was vax'd and no one had immunity and covid was more virulent).
But even more telling than an epidemiological comparison of one nation to another is a comparison of outcomes within nations themselves between pre- and post-vaccination/booster campaign. Prior to the mass vaccination, two parts of the world largely escaped excess deaths from the virus: continental Africa and the Pacific Rim nations. Yet whereas Africa flatlined in terms of COVID deaths throughout 2021-2022, countries like Japan only experienced meaningful numbers of deaths after the mass vaccination program.
Here is a chart of the daily COVID deaths per million in Japan, a country that is super vaccinated (and mask-obsessed).
Notice how Japan is experiencing progressively worse death curves, which only began after everyone (particularly seniors) was boosted, even though Omicron is less pathogenic than the earlier strains. Japan is also the current world leader in cases per million.
Australia is a similar story:
Now contrast these two countries to Nigeria, the most populous country in Africa.
One could assert that there are some unknown factors as to why Africans appear not to die from COVID, compared to the high death rates in North America, South America, and Europe. However, the Pacific Rim countries like Japan and Australia seemed to enjoy almost as low a death rate prior to the booster campaign. After that point, Nigeria (and the rest of Africa) seemed to flatline and be done with the virus, as we would typically expect by now, while the other countries incurred skyrocketing cases and a relatively massive spike in deaths. Obviously, Nigeria’s vaccination rate is much lower than these other countries, but its booster rate is almost nonexistent.
Even within Europe, Scandinavian countries like Norway largely escaped a massive death curve during the first two years of the pandemic. That all changed in 2022. Norway now has the highest COVID death rate per million in the world.
Adding these three Omicron waves together, we see that Norway is beginning to rival the U.S. in terms of death curves. However, America is a much unhealthier country, and America experienced the death curves with the more pathogenic Wuhan and Delta strains.
If you track the number of boosters given per 100 people in some of the aforementioned countries, you will see that the current death curves track almost perfectly in a positive correlation.
Indeed, Chile now has the most deaths per capita in South America, even though the country already suffered a substantial number of deaths and should be done with the pandemic. Nigeria and the rest of Africa indeed are done with the pandemic, and the U.S., which has an average booster rate, is somewhere in the middle in terms of current COVID rates.
So, this is about a lot more than “oh, the vaccines don’t stop transmission.” They appear to proliferate it and also to worsen clinical outcomes. But why?
A group of German researchers tested for which specific antibody levels spike at what time. Specifically, they tested the Pfizer shot against the AstraZeneca shot and discovered something very concerning. Increasingly over time, and particularly with three doses of Pfizer, the immune response switched from the more neutralizing IgG1 and IgG3 antibodies to the non-neutralizing “tolerating” IgG4 antibodies:
High levels of neutralizing SARS-CoV-2-antibodies are an important component of vaccine-induced immunity. Shortly after the initial two mRNA vaccine doses, the IgG response mainly consists of the pro-inflammatory subclasses IgG1 and IgG3. Here, we report that several months after the second vaccination, SARS-CoV-2-specific antibodies were increasingly composed of non-inflammatory IgG4, which were further boosted by a third mRNA vaccination and/or SARS-CoV-2 variant breakthrough infections. IgG4 antibodies among all spike-specific IgG antibodies rose on average from 0.04% shortly after the second vaccination to 19.27% late after the third vaccination. This induction of IgG4 antibodies was not observed after homologous or heterologous SARS-CoV-2 vaccination with adenoviral vectors [emphasis added].
Why is this so important?
Importantly, this class switch was associated with a reduced capacity of the spike-specific antibodies to mediate antibody-dependent cellular phagocytosis and complement deposition. Since Fc-mediated effector functions are critical for antiviral immunity, these findings may have consequences for the choice and timing of vaccination regimens using mRNA vaccines, including future booster immunizations against SARS-CoV-2 [emphasis added].
So not only do these shots fail to produce the first line of defense antibodies known as IgA in the mucosal, something we knew from day one, but even the blood-based antibodies are increasingly the wrong type. This problem seems to get worse over time and with more doses of the shot, which correlates perfectly with numerous studies showing negative efficacy increasing over time, with more doses, and how the vaccinated take longer to clear the virus.
This topic is both very dense and fascinating. You can find clear explanations of this study about IgG4 antibodies in layman’s terms here, here, and here. But the important outcome for us from a policy standpoint is understanding the deadly subterfuge that has been foisted upon 5.5 billion people of the world and how it will be used with many more novel vaccines coming down the pipeline. The medical establishment successfully convinced the world that a vaccine is nothing more than simply stimulating an antibody response and is something that can be done within days of discovering a virus. This is why they now seek to get vaccines approved not based on accurate clinical trials and clinical outcomes but on “immunobridging” – the measuring of antibody levels. Indeed, this is how they got the bivalent booster shots and the JYNNEOS monkeypox vaccine approved and how they plan to get future shots approved.
However, merely measuring antibody levels in the abstract is meaningless and potentially masks harms to the body. God designed our bodies to create the right sort of antibodies, in the right amount, at the right time, in the right place. Any fault in any of those factors can create auto-antibodies, Trojan horse antibodies (antibody dependent disease enhancement) or a misfiring of the immune system, which is some form of original antigenic sin or pathogenic priming that teaches the body to tolerate a specific strain of the virus or respond for a wrong strain. This is why vaccines take years to develop. And this is before we even discuss the fact that these shots are not even vaccines, but are gene therapies that code your body to produce a pathogenic spike that was the result of gain-of-function research and seems to potentially damage every organ system, particularly the cardiovascular system.
In the case of the COVID shots, what the German study discovered is that over time and with increased doses it actually trains your body to tolerate rather than fight the virus it was designed to destroy. The other class of blood-based antibodies are designed to neutralize pathogens; however, the IgG4 class was specifically designed to tolerate innocuous cells (that don’t reproduce) that it repeatedly contacts, such as pollen or peanut particles. They serve an important role and help ensure that people don’t respond with excessive inflammation to everyday encounters with pollen, but to see 20% of the antibody response to SARS-CoV-2 (it was as high as 42% in those experiencing infection after boosters) be something that tolerates it is astounding … and dangerous! In other words, whereas your IgG1 or IgG3 antibodies are like the SWAT team, your IgG4 antibodies are like social workers. You don’t want social workers responding to replicating pathogens like the SARS-CoV-2 spike.
The long-term implications of this study are still unclear, but like every earth-shattering finding, this one will not be studied by governments. If this shot is really upregulating an IgG4 response for most of the population, it could easily explain why herd immunity is out the window with SARS-CoV-2. It’s literally teaching the body to not only respond to the wrong pathogen but to tolerate its existence and not remember to fight it. Also, what does this mean long-term for people who don’t create pro-inflammatory antibodies to defend against pathogens? What sort of damage is being done by not having the virus sufficiently neutralized before it invades the system so deeply?As Kilian Schober, one of the authors of the study, notes (after calling our interpretation of the study too “simplistic”),”Our findings do, however, raise some questions about how to proceed.” But in the past, we used to answer those questions before experimenting on humans, not begin to raise them (and then never answer them) after 5.5 billion people were already injected with the product.
What’s the modus operandi of our dystopian government? Creating a needless deadly crisis, blocking the effective way for dealing with it thereafter, and foisting upon the world instead a dangerous and ineffective way of dealing with it. That might sound a lot like COVID, but it’s largely what officials have been planning for a long time with energy, and now that the population is primed for lockdowns, disruptions, and total authoritarian control as a result of COVID, that is what they plan to do with our energy grid. All for a lie.
This was the coldest Christmas in a half-century in much of the U.S., with many localities setting records, including those not accustomed to the cold like Tallahassee, Florida. Many of us are disgusted at those limiting our natural energy in favor of novel, ineffective energy, thereby causing a doubling or even tripling of home heating bills. But we must also realize that if they had their way, we’d have no heating in our homes at all.
Just like the supposed source of COVID and how to deal with it were lies, our energy crisis is wholly contrived and built upon the lie of global warming. Typically, you would have to make sure we are 100% correct about the “science” behind such irrevocable economic and societal changes before committing civilization suicide by destroying the only reliable sources of energy we have. But in a post-“Great Reset” world, this is par for the course. In fact, the science behind global warming is just as flimsy as the science behind lockdowns, masks, and mRNA shots.
During the Copenhagen climate summit in 2009, chief climate priest Al Gore asserted, “Some of the models suggest … that there is a 75 percent chance that the entire north polar ice cap, during the summer months, could be completely ice-free within five to seven years.” Predictions like this upended our lives with more expensive and more decrepit vital products and services being produced for a generation under the false pretense of taming a crisis that never existed. It turns out that since 2012, the mass of Arctic sea ice is up 31% and Greenland is gaining, not losing, ice. Meanwhile, Antarctica, which was always gaining ice during the period when the Arctic was losing ice, subsequently lost ice last decade and is now regaining it. In other words, the science behind polar ice caps seems to be rooted in the same cherry-picked timing and data as the faux science behind global warming causing either fewer or more hurricanes.
Yet somehow, we are to believe the science is all figured out on how to tamper with global temperatures, just like it was with COVID. Rather than people being more primed to believe in government control after COVID, any thinking person should be even more suspect of official climate lies and the accompanying life-altering policy changes governments want to induce based on them. And boy, would these policy changes be life-altering.
When officials speak of “net zero” for carbon emissions, it means, many times of the year, you would have net zero energy for heating. Picture those nights this past week of below-zero temperatures for much of the nation. Would you want to rely on “renewable energy,” even after billions upon billions in subsidies failed to move the needle on its effectiveness?
At 8am this morning, wind was providing about 1% of the electricity to 13 Mid-Atlantic states and Wash DC.
'Net zero' is how much electricity you will be able to have under climate idiocy. pic.twitter.com/UuMXeQmagA
Temperatures dropped to near zero in Amarillo, Texas, over the Christmas weekend, with wind chills well below zero. Even south Texas faced several nights of once-in-a-generation record cold. Yet even with all that wind blowing, when Texans needed energy most, it was natural gas that held the grid for Texans, while wind and solar collapsed, according to the grid tracking info from the Energy Information Administration.
God might have been sending those wind gusts of 50 mph, but Santa most certainly was not delivering wind energy through the chimney to Texans on Christmas. Now imagine how much better Texas would be doing if the state had invested a fraction of the $66 billion it used for wind and solar in energy sources that actually energize the world rather than in sources that need help from other energy to produce a fraction of the output at a higher cost? Imagine how much cheaper heating prices would be without the global warming mandates and green energy diversions.
If Republican states don’t start looking at how to expand natural God-given fuels and end the green energy scam, the next cold wave could be worse, and we will face energy rationing like the Europeans. For example, depending on the type of job, German regulators now set the thermostats in Germany’s workplaces anywhere between 54 and 66 Fahrenheit. France is preparing for rolling blackouts to close hospitals and schools in a shutdown scenario that could rival the COVID lockdowns used in 2020 to strategically acclimate the public to the new climate of scarcity, pain, and control. Keep in mind, Europe is facing this magnitude of an energy crisis after it has already spent over $1 trillion on “renewable” energy since 2004.
As much as Republicans appear united on energy policy, if you watch carefully, they drop buzz words like a “smarter transition” to “clean” energy and a “better” way of dealing with global warming. Half the Senate Republicans, including Mitch McConnell, just voted to expand an international treaty banning the key coolants in air conditioners, thereby agreeing to the false premise of global warming. Most GOP governors continue to promote tendentious treatment for wind, solar, electric cars, and biofuels that are enabling the dangerous globalist quest to phase out viable energy.
Republicans must end this mealy-mouthed agenda of pursuing a “smarter transition” to green energy, all built upon acceptance of the false premise of global warming. States must audit every regulation that accepts the premise of global warming and harms consumers and work to eliminate it from state policy – be it a law, mandate, subsidy, or regulation.
As we are seeing in Europe, there is no middle ground on this road to the hell of scarcity, which will lead to complete government control every aspect of our lives. In a post-COVID/Great Reset world, there is no longer an excuse to feign ignorance about the “science.” Anyone with working cells in their brain should realize the dark end to that path. The road to a transhumanist hell is paved with “the scienceTM”.
In 2010, Bill Gates famously articulated a four-part equation to reducing the world’s carbon output. Seemingly bizarrely, his first component was reducing the population — through vaccination. “The world today has 6.8 billion people. That’s headed up to about nine billion,” bemoaned Gates in his now infamous TED Talk. “Now, if we do a really great job on new vaccines, health care, reproductive health services, we could lower that by, perhaps, 10% or 15%.” Until recently, I thought this must have been a gaffe. After all, how could vaccines reduce the world’s population? Well, enter the COVID jabs – if you even want to call them vaccines – and we might have our answer.
Questions about fertility issues, stillbirths, and neonatal deaths began to be raised last winter when Scotland experienced a month of higher infant mortality than at any time over the past three decades. Then in the spring of 2022, roughly nine months after most young adults were jabbed with the COVID shots, COVID data analysists began noticing unusual drops in birth rates. The hope was that these numbers were just short-term aberrations due to some unknown transient cause. But months later, the evidence is growing too strong to ignore, suggesting a much longer-term problem, which bizarrely has garnered little concern from policymakers, governments, the medical establishment, or the media. It ranks alongside “died suddenly” both in terms of its magnitude to humanity and the shocking degree of silence in response.
In fact, some media outlets were even celebrating the low birth rates without expressing any curiosity as to the sudden cause. While it’s impossible to prove definitively that the correlation equals causation, it’s stupefying that these shots are not under suspicion given that they are already tied to heart problems, blood clots, massive inflammatory syndromes, and menstrual irregularities and that the lipid nano particles are deposited largely in the ovaries and the testes.
When you are dealing with 1-in-1,000-year anomalies, it takes a civilization-changing event to account for the anomaly. COVID itself cannot be a factor in the sudden drop, because the birth rates were not declining nine months after COVID hit or even in the first year and a half. The other culprit could have been lockdowns, which perhaps disrupted travel, relationships, and cohabitation. But if that were the case, by now we should be seeing a bounce-back effect. Instead, as my friend “Gato Malo” points out on his Substack, the numbers are getting worse.
Sweden is a perfect country to study because it never locked down and should not have been affected socially by the lockdowns. Yet not only did the Swedes experience a sharp decline in births nine months after their vaccination program, the numbers are further deteriorating over time. According to Statistics Sweden, live births are down 8.1% for the year (8.7% per capita), but as Gato observes, the worst month was October 2022 (the most recent month with data), which saw a 13.2% per capita decline. What on earth could explain the fact that this trend is getting worse, other than … you know what? He collated the data from 25 years, and this data, which is in plain sight, raises the question of why there is no policy concern whatsoever.
He further demonstrates that the plummeting birth rates correlate perfectly with the uptake of the vaccines in Sweden among the childbearing population.
Furthermore, any hypothesis as to the cause of the plummeting birth rates would also have to logically account for the rise in neonatal deaths. For example, lockdowns would not explain why the babies being born are experiencing more health problems. The spike protein embedded in the babies’ blood, however, would. Israeli researcher Josh Guetzkow obtained neonatal death data from Israeli health insurance fund Maccabi, which covers 25% of Israelis. He found a tripling of neonatal deaths in two of the quarters post-vaccination.
The timing is very peculiar, according to Guetzkow:
In February, 2021, the Israeli Ministry of Health started to officially recommend COVID-19 vaccines for pregnant women in their 2nd and 3rd trimesters, so the timing of the second quarter spike would coincide with women being jabbed later in their pregnancy 2-4 months prior.
The 4th quarter spike coincides with the booster vaccination campaign in Israel in August and especially September — a drive that aggressively targeted pregnant women. Unfortunately the health insurer claimed not to have information on the vaccination status of pregnant women, so we are not able to differentiate by vaccination status.
This clearly rules out COVID as the culprit, because the neonatal deaths in the earlier quarters in 2020 were low. He goes on to note that this data complements earlier findings he publicized from two major Israeli hospitals showing a sudden increase in stillbirths, miscarriages, and abortions (collectively, SBMA) around the same time. The insurance data does not illuminate the vaccination status of the mothers suffering these reproductive problems, but his earlier data showed a 34% higher rate of SBMAs in Rambam hospital in Haifa among vaccinated women through October 2021.
Obviously, we all understand that you can’t definitively prove causation from correlation, but the lack of any curiosity from the medical community or the government is appalling, especially when the mechanism of action of the spike protein can logically cause these complications (including low sperm count and motility). We have now entered a new era of “speed of science” in which governments can foist novel products upon our bodies with multiple glaring and blaring safety signals setting off alarm bells all over the world, yet until we can prove conclusively the therapeutics are responsible for 100% of the anomaly, they will continue to be promoted. That is completely backward and represents a flagrant violation of the Nuremberg Code.
In a sane world, the makers of these therapies would be behind bars, but instead they are getting a promotion to concoct even more products with this same dangerous technology. Last week, the U.K. announced the formation of a 10-year partnership with Moderna to invest in more R&D for mRNA technology and to build a vaccine manufacturing center that can produce 250 million vaccines a year, particularly for the very problematic RSV shot the company is planning to release next year. In the irony of all ironies, the U.K.’s Health Security Agency will be overseeing this partnership. The UKHSA was the first health surveillance body in the world that published comprehensive weekly COVID updates showing negative efficacy of the shots almost a year and a half ago.
Typically, failure of a corporate partner is an impetus for a government to break the partnership. In the case of vaccines, however, the more they fail, the more they are elevated, subsidized, and even mandated. Unless their definition of failure is the opposite of how humanity would define it.
When it comes to vaccine injury, silence is certainly golden, because it’s the only currency valuable enough to cover up the atrocity of what was done to the entire global population over the past two years. The medical establishment has relied on doctors to turn a blind eye to vaccine injury, allowing those injured to languish without a proper diagnosis and treatment, and continue doubling down on even more doses of this dangerous therapeutic. Thankfully, a few of the former top enforcers of this dogma in the key Western countries of Australia and Israel are making amends for their past misdeeds.
As a lesbian who is married to a woman, a lifelong leader in sex education, former left-wing member of parliament, and former head of the Australian Medical Association, Dr. Kerryn Phelps is not exactly your candidate for right-wing conspiracy theorist. But in a wide-ranging interview with the Chronicle, the Sydney-based doctor publicly acknowledged her own injury as well as that of her partner and divulged how she faced censorship, a lack of treatment options, and a painful journey countless others are facing, a number she says is a lot higher than governments are willing to admit.
“This is an issue that I have witnessed firsthand with my wife, who suffered a severe neurological reaction to her first Pfizer vaccine within minutes, including burning face and gums, paraesethesiae, and numb hands and feet, while under observation by myself, another doctor, and a registered nurse at the time of immunization,” the 65-year-old former AMA president said to the Chronicle.
“I continue to observe the devastating effects a year and a half later, with the addition of fatigue and additional neurological symptoms including nerve pains, altered sense of smell, visual disturbance, and musculoskeletal inflammation. The diagnosis and causation has been confirmed by several specialists who have told me that they have seen ‘a lot’ of patients in a similar situation.”
Phelps noted that the Therapeutic Goods Administration failed to follow up with her reported injury, and many
doctors have told her that not only are they seeing the injuries in droves, but many practitioners themselves were injured but refuse to speak out.
“Regulators of the medical profession have censored public discussion about adverse events following immunization, with threats to doctors not to make any public statements about anything that ‘might undermine the government’s vaccine rollout’ or risk suspension or loss of their registration,” she said.
In other words, there are thousands of doctors who know what is going on, many experiencing it themselves, but who refuse to speak out. Some remain silent; others downright continue promoting the shots. What is quite telling is how even Dr. Phelps herself was still promoting the shots on social media a month after she claims to have been injured by the shots.
For “ineligible for a vaccine”, substitute “inadequate supply of vaccine available for his age group”. #covid19 Profound sympathy for this 15 yo boy’s family as his death has just been confirmed 💔 https://t.co/batoAnRBtD
It demonstrates how entrenched the vaccine cult is and how long it took for even someone injured this badly (along with her partner) to speak out.
The bombshell from Dr. Phelps is significant enough given her biography, but an even more explosive convert to the cause of truth is Professor Shmuel Shapira, who headed the Israel Institute for Biological Research from 2013 to 2021 and literally led the development of Israel’s coronavirus vaccination scheme, in the country that Pfizer referred to as the laboratory for its experimentation. Shapira has been speaking out against the shots for months, but not after he was personally injured by his third dose. Last week, he wrote a series of tweets describing his conversion:
I was wrong 3 times: * In the first shot * In the second shot * and in the third shot Who said that those who are injected do not admit that they were wrong?
The pigs from the animal farm, got time off for the final and were sent to trash. I touched them at a painful point. Yes then I will repeat it, I was wrong 3 times when I was injected the first, second and third time. Unlike the dwarfs, I'm proud of everything I've being doing.
Why aren’t others speaking out? Well, when even the man who was almost the Fauci of Israel gets this much blowback, it’s no wonder few have the courage to fight.
You have no idea what a campaign of slander and anonymous threats I go through. Some of it is quoted to me by journalists and others. The traces clearly lead to what used to be the Ministry of Health ,but not only to him. They aren't even smart enough to clean a fingerprint.
What this means is that there are likely a great many others who know this is going on – perhaps from personal experience – and yet, like a death cult, they will not admit they were wrong. They are trained to find only medical ailments they are primed to look for. If it’s not in their memorized and regimented protocols, then it doesn’t exist. The medical system has become so monotonized and streamlined that almost no doctor is willing to even cognitively question the hierarchy, much less articulate opposition.
This code of silence would be bad enough if the vaccination campaign were over and it was just an issue of treating those already injured. Yet the pressure and even mandates still exist in some settings, and almost all doctors still promote the vaccines. Furthermore, they are pushing mRNA technology for flu and RSV shots as early as next fall.
Silently accepting this degree of short-term and unknown long-term risk would be bad enough if the shots actually worked against COVID. But as we’ve known for well over a year and a half, the more you inject, the more you infect. The latest evidence is from a Cleveland Clinic preprint study of over 50,000 of CC’s in-house health care workers. The retrospective cohort study shows a strong positive correlation between an increase in vaccine doses and a stronger likelihood to test positive for the virus. The unvaccinated performed the best, and the boosted were three times more likely to get infected.
This is just over 90 days. We’ve seen in the past from other studies that the negative efficacy intensifies over the months, which might explain why for the first time in history this virus shows no signs of going away, except in Africa, where few people were vaccinated. Last year, long before the negative efficacy of the shots associated with Omicron that we are seeing today, Sweden conducted the most comprehensive long-term study of vaccine effectiveness in the world and found that after six to seven months, “no effectiveness could be detected” from the Pfizer shot. In fact, the study found negative efficacy after 210 days for those over 50, which harmonizes with what we are seeing before our very eyes throughout the world. For some older adults, the shots are as much as -77% effective, and the numbers seem to drop every month.
Shockingly, this cycle of failure allows the same duplicitous doctors to fearmonger even more people into getting even more doses, perpetuating and exacerbating an endless cycle of viral immune escape, mutations, and pathogenic priming that leads to negative efficacy reflective of suboptimal antibodies and a leaky vaccine.
For months, Walgreens has been posting the results of its weekly COVID testing by vaccination status. They have consistently shown the unvaccinated to have the lowest number of cases relative to the number of tests (the unvaccinated are subjected to more testing mandates in the workforce).
As you can see, the unvaccinated have the lowest positivity rate. It’s also self-evident that the negative efficacy intensifies over time since the duration of the last dose. And even the Omicron boosters, which were tested on eight blind mice, are now addressing a variant that is nearly extinct. According to the CDC, BA.4 is extinct and BA.5 represents only 10% of cases and is rapidly declining.
Yet the FDA just approved these extinct, dangerous, negative-efficacy shots for babies! It’s no longer a tenable position for Republicans to merely oppose mandates. Mind you, so many red states still have mandates on health care and in public colleges. They must completely stop promoting the shots, oppose any future mRNA shots under the current design, sponsor treatment for those injured, create state-based vaccine reporting, and encourage rather than punish doctors to speak out and dissent. “See something, say something” needs to be the catchphrase in the medical profession. Too many lives are on the line to remain silent.
The time has come for a coalition of governors, attorneys general, and state legislators to demonstrate the power of broad-based federalism to interpose against extreme federal tyranny.
Many conservative commentators have finally woken up to smell the stench of the Fourth Reich following Biden’s speech targeting political opposition, reminiscent of the authoritarian language of past dictators. However, they should have been awake since March 2020, when our government declared de facto martial law on our lives, liberty, and property and used our bodies as lab rats with an ever-growing list of experimental therapies. They should have awoken from their slumber after Americans were targeted with solitary confinement and disproportionate punishment for zero or nebulous crimes at the Capitol on January 6, after months of killing, rioting, and looting by BLM with impunity.
If Biden’s speech is really to be a turning point in this one-sided cold war that is heating up, conservatives should resolve to use the power they already wield over Republican governors and demand united action for states to protect constitutional rights from this thuggish Biden administration and national security deep state apparatus that threatens our liberties more than any foreign enemy in our history. Rather than making idle promises of winning back the House with RINOs or winning back the presidency years from now when it’s too late, we should be demanding action now from 20 or so GOP trifecta-controlled state governments. If they fail to take action now, then the entire point of federal elections with divided government is moot.
What would a coalition of federalism look like? A group of prominent governors, attorneys general, and state legislative speakers and majority leaders would initiate a declaration in one state – let’s call it the “Miami Declaration,” for example. The declaration would lay out a list of grievances and examples of the federal government violating the rights of the individual: from medical freedom and bodily autonomy to privacy infringement, collusion with big tech against First Amendment rights, and using federal agencies to persecute political opponents. The declaration would pronounce these states to be constitutional sanctuaries that protect all constitutional rights, including against the federal government. Here are just a few ideas that should be contained in the declaration:
Criminalize the enforcement of any federal COVID mandate – whether by a federal, state, or private actor – within the boundaries of the states. This would include so-called federal lands within the state.
Order all education and health care institutions within the state to stop complying with recent edicts on transgenderism or COVID with the threat of severe fines.
Block the distribution of any new vaccines that have not been properly studied.
Create a commission to study who is responsible for the COVID response and the botched therapeutics, along with an audit of what other therapeutics are in the pipeline that violate bioethical norms.
Nullify onerous federal regulations on energy and mineral exploration and production within the coalition of states so that states can begin protecting their residents from the coming nuclear winter on energy use.
Impose severe penalties on tech companies that censor political opponents of the regime until they come clean on the scope of collaboration with the federal government against these individuals.
Provide legal and financial backing to those political dissidents being targeted by the federal government primarily for their political views.
Suspend all training and cooperation between state and local law enforcement and the federal alphabet soup agencies.
Even if Republicans refuse to block funding for the vaccines, Paxlovid, and Ukraine – most likely because they agree with Democrats on those issues – they should at least withhold support until the extra funding for the IRS is kept out of the bill. Fighting overzealous taxation, especially when it is politically targeted, was always a universal value of the Republican Party. The IRS waited until Friday afternoon before the holiday weekend to admit that information from 120,000 form 990-T filers was inadvertently posted online due to “a human coding error.” These means the names, contact information, and financial information of about 120,000 people who have IRAs in non-security assets were breached. Does anyone really trust that the IRS is telling us the whole truth?
From now until the election, Republicans will seek to distract us with flaccid promises of deliverance in the future. The best way to verify their sincerity is by demanding that they actually use the power they currently hold to counter deeply destructive and unpopular policies from this regime.
Imagine a doctor refusing to treat a patient until he stops engaging in orgies that put him at risk of contracting monkeypox. Well, he would be following the science and data a lot more than those refusing service to those who don’t get the shots or wear masks, but unlike in the latter cases, that doctor would be out of a job and up to his neck in civil rights lawsuits. The time has come to even the score on discrimination and human rights.
Rayne Barton of Elizabethtown, Pennsylvania, doesn’t have the luxury of avoiding the doctor. With diabetes, chronic heart problems, kidney disease, and spinal stenosis, Barton needs to constantly see doctors and get prescriptions refilled. Yet, as the Epoch Times reports, she has been banned from all Penn Medicine facilities since Feb. 17, 2022, because of mask disputes. On July 22, Hypertension and Kidney Specialists, an independent doctor’s office in Lancaster, called the police on her after she was told to leave the premises during a mask dispute. She was forced to ride in the back of a police car with her hands behind her back, despite her painful back condition.
How is this allowed to happen in America? How can a policy as inhumane, immoral, and illogical as covering one’s breathing holes be allowed to stand after being repudiated for two and a half years? How is free breathing not a basic human right, especially for those with disabilities, or at least covered by the Americans with Disabilities Act and anti-discrimination law? Companies often spend millions of dollars complying with ADA requirements for customers, yet here they can discriminate against trauma victims when it costs them nothing and when they are free to wear masks themselves if they believe they work, a proposition refuted by the very reality of the virus still spreading unrestrained in all of the most masked places in the world.
Most Americans are no longer affected by the masks because the powers at be smartly lifted the mandates for the majority of people headed into the election. But for people affected the most – those with disabilities needing to see the doctor often – it is still a devastating human rights violation. And unless we extirpate this inhumane treatment from our society, it will be reinstated on all of us intermittently.
The Epoch Times reports that Barton is incapable of placing a mask over her face because she is a victim of childhood trauma. She was attacked by a group of boys as a kid and had dirt stuffed down her mouth, which is why she can’t cover her mouth to this day without it triggering a panic attack. Even for medical interventions that have scientific rationale (and don’t have the option of others utilizing it, as does mask-wearing), we always make exceptions for those with disabilities. What has become of us as human beings that we are still engaging in this sort of behavior long after the “my mask protects you but not me” absurdity has been thoroughly debunked?
The time has come to codify medical discrimination into civil rights and ensure that nobody can ever be denied treatment on account of not getting a shot or wearing a mask. There is never a scientific or moral rationale for such a requirement, and it is clear that it is all promoted through the misinformation propagated by the federal government. Masking only became a thing because of government intervention; it therefore must be uprooted with a display of state government power.
The slate is not clean when it comes to the private sector and discrimination law, especially in something like medical treatment, which is often (especially in a hospital) designated as a public accommodation. They cannot discriminate against people even when their behaviors are proven to cause their ailments. Can hospitals turn away the recurring patients who are on their third drug overdose in as many months? Can they refuse to treat the gunshot victim who himself had been involved in multiple gang shootings? Can they deny treatment for monkeypox if the patient attended a super-spreader orgy that is almost exclusively responsible for the spread of the virus? Until they can, there is no moral or scientific rational for allowing doctors to deny organ transplants to people without shots or care for people who don’t cover their human breathing holes.
Emerging from the past two years of COVID fascism without instituting major legal and political protections against abuse of bodily autonomy would be like not addressing box cutters on planes after 9/11. Yet few Republicans care to act. They have a pre-March 2020 mindset about what we face in government, the medical cartel, and the globalist entities like the World Economic Forum and the WHO, all manipulated by China in the background. Policymakers are slyly choosing to subject only medical facilities and the military to continued regulations so as not to enrage the majority of the electorate, but make no mistake, those people are worth fighting for. Also, we will all continue to suffer from assaults on freedom if we don’t push for new civil rights concerning medical freedom. Such a plan would include:
Updating the Civil Rights Act of 1964, so that employers, retailers, hospitals, schools, and others would not be able to discriminate against individuals based on refusal to wear a mask or get a shot, just like they can’t discriminate based on sex, race, or religion. We the Patriots USA has delivered a petition to do just that to all the members of Congress. Red states with supermajorities could easily do this on the state level next session.
Subject anyone who forces someone to wear a mask or get a shot to liability for damage from masks or shots.
Threaten the nonprofit status of any hospital that engages in such discrimination.
Pass a patient bill of rights.
Pass a digital health privacy bill of rights.
Remember, none of these policies organically emerged from the free market. They were all ultimately mandated or manipulated by the federal government. States must fight power with power. If we had a true free market, even a minority of doctors who don’t believe in masks would be able to advertise and place themselves on a list for people like Barton to use. But they would be targeted for loss of board certification or even state medical licenses.
It is shocking that even as the Biden administration declares a second public health emergency on top of COVID, Republicans have not even made reversal of these policies a centerpiece of their campaign platforms. Let us not forget the admonition of founder John Dickinson: “All artful rulers, who strive to extend their own power beyond its just limits, endeavor to give to their attempts, as much semblance of legality as possible. Those who succeed them may venture to go a little farther; for each new encroachment will be strengthened by a former.” COVID fascism must be destroyed – root and branch – if we are to have a shot at precluding the next wave of encroachments on our bodies.
Few people in America were following the passage of the $280 billion handout for huge chip manufactures and the 5G industry, but the politics surrounding the bill, as well as the bill itself, perfectly exemplify the “uniparty” dynamic. To begin with, GOP leadership had no problem with this corporate welfare bill and worked together to craft it. However, McConnell promised to hold up the bill unless the Democrats committed to forgoing budget reconciliation, a process through which they can pass liberal priorities without the need for 60 votes. Well, McConnell and 17 other Republican senators eagerly provided the votes for the “chips-plus bill,” and Schumer responded by announcing his plans to pass budget reconciliation to remake our economy!
Leftists love over-taxing and over-regulating certain businesses while granting endless corporate welfare to other industries in order to create transnational monopolies. The semiconductor and 5G industries embody everything conservatives are worried about with the corporate masters – ties to China, privacy concerns, health concerns, outsourcing American jobs, creating monopolies, and funding woke global corporations that hate our values and use the funding as well as the technology against our best interests.
In comes the “chips and science” bill (HR 4346), a $280 billion package for the science and tech cartels that includes $54 billion in five-year grants for manufacturing and design of semiconductors and 5G wireless deployment, plus $24 billion in tax credits for new semiconductor manufacturing facilities through 2026 and funding authorizations to bolster U.S. scientific research. These are some of the wokest and wealthiest companies. Intel, which aggressively lobbied for the bill, already earned $79 billion in revenue last year. Yet 17 Republicans, including Leader McConnell, joined every Democrat sans Bernie Sanders and voted for this earth-shattering and expensive bill with lightning speed.
Even if one agrees there is a need to somehow pick winners and losers, we should have at least secured provisions ensuring that China can’t steal our technology, that the jobs and supply chain remain here in the United States, and that these companies can’t promote wokeness, and we should have addressed oversight issues of privacy and health concerns with 5G. Rather than addressing the insane regulatory burden that has broken our domestic supply chains, this bill will further incentivize and invest in the current globalist system that sells out America to China. Absent large-scale policy reforms, more funding of supposed “American” tech giants is tantamount to funding China. The GOP’s answer to everything we don’t like is to add more spending to it.
To make matters worse, in the final days, the bill added hundreds of pages and hundreds of billions of dollars to fund the broken “science” agencies that should be shuttered. This includes a five-year $102 billion authorization for the National Science Foundation, Commerce Department, and National Institute of Standards and Technology to increase investments, which represents a $52 billion increase in baseline spending of these bloated and unnecessary agencies. It also includes billions of extra funding for “basic energy sciences” and “environmental sciences.” It appears that McConnell and company still “trust the science.”
In other words, even in the minority under a very radical and unpopular Democrat regime, Republicans think that the base spending bills weren’t enough and desire to increase funding for everything that is wrong with government. Republicans will wax poetic today about inflation, yet when it came to the issues that mattered – COVID, Ukraine, and now a massive Big Tech bill – they not only fail to filibuster big budget bills, but they will even vote for new massive spending bills while in the minority. At least in the past they used to be righteous in the minority and screwed conservatives only after winning elections.
Although there are some House Democrats who are at least consistent in their hate for big business and will oppose this corporate welfare, Republicans plan to supply the votes.
A source on Capitol Hill tells me 10 Democrats are opposed to CHIPS…
But 38 House GOP plan to vote yes & put this bill over the top.
— Scott T. Parkinson (@ScottTParkinson) July 27, 2022
This is part of a broader betrayal of passing red-flag laws, flirting with gay marriage, and passing an NDAA funding the woke and broke military that is mandating the shots on soldiers.
To add insult to injury, McConnell originally promised that if Democrats didn’t give up on plans to pass budget reconciliation, he would block passage of the chips bill. A budget reconciliation bill is the only maneuver by which Democrats could attempt to ram through a transcendent policy change without facing a filibuster, assuming they keep every Democrat senator in line. Yet McConnell then votes for the bill, and within hours of its passage yesterday, Senate Majority Leader Chuck Schumer announced plans to pursue a reconciliation resolution.
After months of a stalemate with Senator Joe Manchin, Schumer announced plans to pass a $370 billion “climate and energy” bill, funding the Great Reset, three years of subsidies for the health care cartel under Obamacare, and more handouts for Big Pharma. They are calling it “the Inflation Reduction Act of 2022” because it purports to pay for the spending with tax increases, and somehow that would reduce inflation.
Note that McConnell said he would blow up the chips bill if Dems tried to do budget reconciliation pkg for social spending plan. Chips passes. Manchin/Schumer immediately announce agreement on reconciliation measure
Thus, when Democrats pass that bill next week and all these same McConnell Republicans vote against it, just know that McConnell gave up his leverage and is responsible for that massive tax-and-spend giveaway to woke industries because he agreed to pass another massive corporate welfare bill. Nor do they have any plans to hold up the NDAA or the fiscal year 2023 budget bill when it comes due at the end of September. But fear not. Spend the next few months campaigning for this same party so that none other than a Majority Leader Mitch McConnell is waiting for you as the reward for your hard work.
Can Congress pass a law requiring that all platforms of speech censor any negative comment about Pfizer? “Well, of course not,” you will say, “it violates the First Amendment.” In that case, why should it be different when the executive branch works intimately with government-created and liability-protected monopolies to zap anyone’s Twitter account who is critical of Pfizer and its magical products? That is not free market or private enterprise; it is the worst form of fascism, and now a new federal court ruling might bring this point to life.
On Tuesday, a federal judge in Louisiana granted the request from the Louisiana and Missouri attorneys general for discovery to collect documents linking the Biden administration to social media censorship. Thanks to this important order, we might be able to discover the scope of collaboration between government and Twitter and Facebook to censor stories (and people) pertaining to the Hunter Biden laptop story, the origins of COVID-19, the efficacy of masks and lockdowns, and election integrity.
On May 5, Missouri AG Eric Schmitt and Louisiana AG Jeff Landry filed a First Amendment complaint against the Biden administration in the Western District of Louisiana alleging that the administration violated the Free Speech Clause by working with the tech giants to label all dissenting viewpoints on the aforementioned issues as “misinformation.” They alleged that this effort is being led by a “Disinformation Governance Board” (“DGB”) within the Department of Homeland Security.
In Judge Terry Doughty’s Tuesday order, he ruled that the states have standing to bring the claim and in an effort to buttress their request for an injunction against the federal collaboration in censoring private political views, they can request information from the Biden administration proving or disproving their allegations of collaboration with social media companies. The administration has 30 days to turn over the documents.
It’s already in the public sphere that the Biden administration has been leaning into social media censorship in numerous ways. Here are just a few examples:
In a March 15, 2020, email with Dr. Fauci, Facebooks’s Mark Zuckerberg proposed to coordinate with Fauci to “make sure people can get authoritative information from reliable sources” and proposed including a video message from Fauci because “people trust and want to hear from experts.” Remember, as a candidate running for president, Biden suggested that Facebook should be subject to liability for not censoring views he deemed harmful.
On May 5, 2021, former Biden press secretary Jen Psaki stated, “The president’s view is that the major platforms have a responsibility related to the health and safety of all Americans to stop amplifying untrustworthy content, disinformation, and misinformation.”
On July 15, Psaki went a step further and acknowledged the collaboration in private. “We are in regular touch with these social media platforms, and those engagements typically happen through members of our senior staff,” she revealed. “We’re flagging problematic posts for Facebook that spread disinformation,” she added. This was a direct admission that what was going on behind the scenes was old-fashioned government censorship, which clearly violates the Constitution.
After that press conference, Facebook responded to the pressure by acknowledging that “the company has partnered with government experts … to take ‘aggressive action against misinformation about COVID-19.’”
The following day, Psaki took it to the next level by suggesting that the various social media companies should be collaborating with each other to ban anyone from all the platforms after being removed from one. “You shouldn’t be banned from one platform and not others … for providing misinformation out there,” she declared. This is also the same day Surgeon General Vivek Murthy posted a misinformation advisory laying out the parameters for social media platforms to censor information on COVID and its policies.
Then of course we all remember in February when the Biden administration directly called on Spotify to censor Joe Rogan for having doctors on his show who were successfully treating COVID.
Finally, let’s not forget that the White House singled out 12 private individuals to be targeted for censorship as the “disinformation dozen.” We also know that private emails released via FOIA revealed that the CDC Foundation worked with Facebook, Merck, the WHO, and other pharma entities on an “Alliance for Advancing Health Online” initiative to control the narrative.
Thus, it doesn’t take a genius to realize that there were likely some juicy conversations going on between the tech executives and the Biden administration, probably in concert with the pharma companies, to silence all opposition. When you have the president demanding such censorship and warning that the opposing viewpoints are “killing” people, the entire argument of “private” companies being able to do what they want goes out the window. As Justice Thomas wrote in a 2021 case, it is indeed a First Amendment violation “if the government coerces or induces it to take action the government itself would not be permitted to do, such as censor expression of a lawful viewpoint.”
Thankfully, it appears that this judge saw through the high-tech modern version of censorship for what it is – pure fascism.
While the legal dispute plays out in court, it’s time for conservatives in the legislatures to hit back at the RINO governors for continuing to act as if anything COVID-related – be it a vaccine or mask mandate – is somehow coming from the private sector. The government mandated it for some, censored opposing viewpoints, absolved pharma of liability, paid for the product, distributed it, and marketed it. The notion that private actors endorsing these policies is an exercise in free-market capitalism is absurd. It is the responsibility of the state to interpose against such tyranny by banning companies from joining in with the federal policies.
We saw this done very effectively when the Florida Department of Health recommended against the baby shots and refused to distribute them. Publix actually decided on its own to follow the guidance of Florida rather than the federal government. It demonstrates that so much of this enforcement in the private sector is being done with the federal boot on companies’ necks. Those Republicans who hide behind affinity for the “private” sector and free markets to allow federal tyranny, censorship, and persecution to continue are complicit in the worst form of fascism. The fact that private monopolies get roped into government fascism doesn’t ameliorate the pig; it makes it even more dangerous.
It’s the body of government closest to the people, yet it’s the most forgotten, overshadowed, and weakened body in recent years. However, with the Dobbs opinion returning the power to regulate abortions to state legislatures, we now have the opportunity to focus our attention on legislative elections, sessions, and policies and settle our acerbic cultural and legal differences in the most prudent and democratic process.
We are an irrevocably divided nation, and it will only get worse over time. We can’t agree on the definition of a marriage, a woman, a citizen, a criminal, a fundamental right, or the purpose of our existence, much less the purpose of our government. We can either continue forging ahead with a winner-take-all approach to politics and have the federal executive bureaucracy – the least accountable and transparent branch of government and most distant from the people – decide every important political question. Or we settle those debates in state legislatures – the branch closest to the people where most members are elected every two years.
Whether you abhor abortion as murder or think it’s the greatest sacrament of virtue, the reality is that red states are going to ban abortions (many already have) and the blue states are going to obsessively expand access to them. Unlike the seven justices who initially banned all regulation of abortion in 1973, all those legislators in each state will be subject to removal every two or four years. For the most part, the legislators will vote in a way that reflects the values of the majority in their areas. This is the self-sorting process we’ve always needed. This dynamic needs to expand to every other important issue of our time. It’s not a perfect process, but it’s much better than where we are today, and it will allow us to live side by side harmoniously in a de facto amicable separation, albeit with shared custody over certain issues that are national in scope.
In the coming months, conservatives will be trained by their favorite Fox News media figures to obsess about the potential of a RINO takeover of Congress and the coming presidential election, even though the latter won’t even be relevant, policy-wise, until 2025. But the reality is that Republicans control trifecta supermajorities in a number of states today and will only expand that dominance next year. Come January, they have the ability to make those states de facto sanctuaries for our rights and values – if only we focus our pressure on elected state Republicans and educate them concerning the enormity of their power. It’s time to use it.
In his national design for governance, Madison explained the state vs. federal arrangement in Federalist #45 as follows:
“The powers delegated by the proposed Constitution to the Federal Government, are few and defined. Those which are to remain in the State Governments are numerous and indefinite. The former will be exercised principally on external objects, as war, peace, negotiation, and foreign commerce; with which last the power of taxation will for the most part be connected. The powers reserved to the several States will extend to all the objects, which, in the ordinary course of affairs, concern the lives, liberties and properties of the people; and the internal order, improvement, and prosperity of the State.”
Think about issues like COVID fascism and transgenderism. Internal order, liberties, and property, etc. – this can all be rectified at a state level. Anything outside war and foreign commerce is fair game. This is where conservatives failed to act during the lockdowns and COVID fascism. They should have activated the legislatures immediately and forced debate for the states to immediately reject the federal policies. It’s still not too late to change course.
In responding to the Biden administration’s immoral and illegal policies and edicts over the next two and a half years, conservatives should have a one-track mind and be singularly focused on how they can pressure their legislatures to interpose against the federal tyranny. Conservatives have long been distracted away from a state legislative focus, but perhaps the Democrats will teach them how it’s done. Believe me, the blue states will immediately take action and juice up funding for abortion while expanding its legal scope – perhaps even to after the birth of the baby.
Likewise, most GOP legislatures and attorneys general seem to have acted swiftly to immediately ban abortion at the first opportunity. But we now need to see this swiftness on other issues as well. For example, Biden’s Department of Education just promulgated a rule putting any school or university on the hook for sexual harassment if they don’t call men who think they are women by female pronouns. This is the sort of illegal federal regulation that states must immediately stop. Legislatures should instantly convene and block its implementation within their states.
The big problem we have in legislatures, though, is that so many of them are only in session for a few months a year. In states like Texas, they are only in session every other year. This means that, for example with COVID, when you have federal and state executive branches suspending the republic, we often have to wait months or years for legislatures to act. It was OK to have a part-time legislature when we had a part-time executive branch and the legislature was the only organ of government that legislated. However, now that the federal and state departments of health and education legislate 365 days a year without any checks or balances, the concept of a part-time legislature actually harms us.
As such, conservatives must begin pushing reforms to make it easier to call legislatures back into session, and it should not be tied to the whims of the governors. We don’t need state legislatures voting on bills all year, but we must reserve the prerogative to get them back into session at a moment’s notice to interpose against tyranny.
For years, Republicans have accumulated a ton of power in many states, have done nothing with it, and have failed to clean up their own cultural Marxist swamps within state-run agencies. Abortion was the only red line conservative voters established and held their elected representatives to. It succeeded beyond our wildest dreams. Now it’s time we harness that energy for issues like medical freedom, Pfizer liability, transgenderism, illegal immigration, crime, First Amendment protections, and interposition against the tyrannical Biden administration. What the Dobbs victory has clearly shown is that we will only enjoy the rights and policies commensurate with our desire to fight for them.
They did this under the guise of science and saving lives. We now have a generation of children who are delayed in language, social skills, and educational attainment, while overburdened with mental, emotional, and behavioral ailments. And yet it was all done for absolutely nothing – no gain, all pain. This has been appallingly obvious since schools were shut down and then children masked in 2020, but a new study from Sweden – the global control group – demonstrates the scope of this crime with unmistakable clarity.
A study by Swedish researchers published in the International Journal of Educational Research found that in this Nordic country, “word decoding and reading comprehension scores were not lower during the pandemic compared to before the pandemic.” This is simply astounding, given what we have witnessed in almost every other country. The researchers analyzed 97,000 Swedish primary school children from 248 different municipalities, 1,277 schools, and 5,250 classrooms.
Just contrast this to a McKinsey study that analyzed more than 1.6 million K-12 students in over 40 U.S. states that found that students were, on average, five months behind in mathematics and four months behind in reading. An investigation by WBFF’s Project Baltimore from the local Fox affiliate found that 62% of middle schoolers in Baltimore County had one or more failing grades by the third quarter of the 2021 school year, up a whopping from 35% from before the shutdowns. Investigators also found that 41% of Baltimore high schoolers had a grade-point average of 1.0 or below, an increase of 24% since before the school closures in March 2020. The education situation in a state like Maryland is so dire that 81 percent of all Maryland students tested last year in grades three through five were not proficient in math, and 76 percent were not proficient in English language arts.
It makes you wonder if Swedish kids might outshine American children one day in English in addition to their native language! What was the secret to their success? They simply followed science and morality and kept schools open without dystopian plexiglass and masks. There was no fearmongering, social isolation, learning impediments, or learning stoppages. And of course, there is no evidence that a single child died from COVID as a result of schools being open. All gain and no pain.
In the light of international studies on reading skills in younger students during the pandemic, we conclude that the decision to keep schools open benefitted Swedish primary school students. This decision might also have mitigated other potentially negative effects of school closures, especially for students from more disadvantaged backgrounds.
Never before in our history has there been such a grave policy promulgated by government that was known up front to have no benefit but induced cataclysmic damage. It’s not just the learning disorders that are plaguing a generation of kids. A 2021 paper in the Lancet found, based on data from 204 countries, a 27.4% increase in major depressive disorders globally, accounting for an additional 53 million cases. Additionally, researchers found a 25.6% increase in cases of anxiety disorders, accounting for another 76 million cases globally.
One cannot possibly quantify the long-term effects to society of driving such a ubiquitous mental and emotional health crisis. According to the CDC, a third of high school students reported poor mental health during the pandemic, and 44% said they “persistently felt sad or hopeless.”
What is going to become of those kids? Many of them will live unproductive and sad lives, but many others will die young. A paper published recently in JAMA found that the rate of drug overdose deaths doubled among adolescents during the pandemic. In 2019, the overdose fatality rate among adolescents was 2.36 per 100,000, very consistent with the previous decade. In 2020, it shot up to 4.57 per 100,000, and for the first six months of 2021, the rate increased another 20%, to 5.49 per 100,000.
Kids should never have been made to feel anxious about the virus or about the response to it because it should never have affected them. It was known early on that not a single one of Sweden’s nearly 2 million children died of COVID during the initial wave in the spring of 2020 when Sweden kept its schools open (without mask requirements) and the rest of the world shut their schools.
Rather than admitting their mistake and committing to never shutting down schools again, governments are once again foisting a policy with all pain and no gain on the youngest of children. Later this week, the FDA will likely approve Moderna’s and Pfizer’s outdated shots on babies and toddlers, for a virus that never harmed them. We have never pushed novel therapies on children, especially those who already have numerous documented problems, for something that poses such a low risk, especially when the vaccine is outdated and doesn’t work for the variants circulating today.
As of June 3, there were already 49,878 children (ages 0 to 17) reported in VAERS who have experienced an adverse event from one of the COVID jabs. 7,547 of the childrenwere hospitalized, and 125 died. Remember, this is for a virus that no longer exists in that original form and from which there was a near-zero risk to children.
Between March 2020 and December 2021, according to researchers from the U.K. Health Security Agency, even among the rare documented pediatric COVID deaths, 56% of those under age 20 “were due to unnatural causes or due to causes unrelated to COVID-19.” Even among the remaining 81 deaths in the entire country under age 20, 75% had significant co-morbidities. Yet we are giving them a novel therapy Pfizer itself admitted is associated with hundreds of adverse maladies based on de facto zero risk, just like we shut down their classes, socially isolated them, and mummified their faces for the same nonexistent risk. What will it take to suspend these immoral experiments on our children?
Next week, the FDA Vaccines and Related Biological Products Advisory Committee will meet to likely offer emergency use authorization for Moderna and Pfizer’s biological products to be injected into babies as young as six months old. No amount of evidence demonstrating negative efficacy and enormous side effects will factor into its decision. Never mind the fact that there never was an emergency for young children to begin with, and there certainly isn’t one now.
Yet the FDA will undoubtedly approve a shot that has failed and is outdated – so much so that two weeks later, it will meet about updating the formula for new variants, of course, after having injected the outdated formula into the arms of babies and toddlers. One data point that certainly will be missing from the meeting is the observation about Portugal.
According to Statista, Portugal has the highest vaccination rate of any country in Europe aside from the tiny island of Malta. Nearly every adult is vaccinated in this nation of 10.3 million, 94% of all people (including young children) have received at least 1 dose, and 70% have received boosters. In fact, the New York Times ran an article about Portugal last year, noting that “there is no one left to vaccinate” there.
Yet, Portugal now has the highest case rate and COVID death rate per capita in Europe and the second highest COVID fatality rate in the world behind Taiwan, according to Our World in Data.
Here is the case rate map of Europe:
And here is the death rate map:
At 2,293 cases per 1 million individuals, as of June 7, Portugal’s 7-day rolling average case rate is seven times greater than that of the United States and is now higher than the worst peak of cases in America. Moreover, it’s not that Portugal never had a big wave – it has already experienced a peak in the winter that was three times as great as the worst days in the U.S. So even after many people already had the virus, officials keep testing positive for the virus despite – or perhaps, because of – the near universal vaccination rate.
It is true that Portugal has a high rate of testing, but not that much higher to account for exponentially higher case rates. As of June 1, Portugal’s positivity rate was nearly four times that of the U.S.
Then there are the COVID deaths. At 4.1 deaths per million, Portugal is now far outpacing all the other European countries with high case rates by over 60%. Its current death rate is more than four times that of the U.S. This simply should not be happening now that everyone is vaccinated and everyone who is vulnerable is boosted if the shots are anywhere near as effective as we are told.
The Portugal News reported that between May 24 and May 30, the southern European nation “recorded 175,766 infections, 220 deaths associated with COVID-19, and an increase in hospitalizations and intensive care.” Health Minister Marta Temido said last week that “Portugal is probably the European country with the highest prevalence of this sub-lineage and this partly explains the high number (of cases) we are seeing.”
But that really doesn’t explain it. Why would Portugal have a much worse problem with these variants than the country in which they were first detected — namely South Africa? Is this not a fulfillment of Dr. Geert Vanden Bossche’s warning that the sub-optimal evolutionary pressure of these shots, originally designed for the Wuhan strain, would work against the body for future variants?
Let’s a take a look at South Africa’s BA.4/BA.5 wave from late May as compared to Portugal’s? Can you even detect it?
South Africa’s recent peak, which is now over with, was one-twentieth the size of Portugal’s – and this is after Portugal already had exponentially more cases from the previous wave. However, even as it relates to death rates, the afflicted country is outpacing South Africa.
Keep in mind that Portugal is still experiencing higher death rates even after having already incurred a lot of deaths from the original pool of vulnerable people during the first winter. It simply makes no sense for Portugal to be experiencing this many deaths with Omicron, which does not replicate well in the lungs. Remember, while Portugal has run out of people to vaccinate, according to the New York Times, less than a third of South Africans are vaccinated with very few having had boosters. Also, South Africa’s life expectancy is 18 years lower, and 20% of the population has AIDS.
For how much longer is the FDA going to be allowed to ignore a year’s worth of signals not just indicating cataclysmic safety concerns but negative efficacy – and downright perpetuation – of the virus? Just look at this week’s Walgreens COVID-19 testing index, and you can once again see that higher positivity rates are associated with those with more shots, especially as time goes on.
The mendacity of obfuscating the truth about these shots has gotten so ludicrous that the media and medical associations are now chalking up the rash of sudden cardiac deaths among young people as an unexplained “sudden adult death syndrome.” And now they want to inject these products into the final group of unvarnished children. What does that say about who we are as a people if we let it happen?
In the New York Times article from October crowing about “no one left to vaccinate” in Portugal, Laura Sanches, a Portuguese clinical psychologist, is quoted as bemoaning the fact that Portugal doesn’t “really have a culture of questioning authorities.” Well, here in America, we once did have such a culture. Reagan once said that “freedom is the right to question, and change the established way of doing things,” an understanding “that allows us to recognize shortcomings and seek solutions … to put forth an idea, scoffed at by the experts, and watch it catch fire among the people.” Will we finally exercise that freedom?
It’s truly hard to overstate the damage done to a generation of children by the two-year masking regime. From language and developmental inhibition to social and behavioral anxiety, these Chinese cloths have created a generation of bumbling fools. So, was it worth it?
In a preprint published in the Lancet, Ambarish Chandra of the University of Toronto and Tracy Beth Høeg of the University of California at Davis replicated a CDC study comparing counties with school mandates to those without mandates. However, rather than using the CDC’s artificial and arbitrary number of counties and duration of study, they extended the study using a larger sample of districts and a longer time interval, employing almost six times as much data as the original study. Using this updated method to measure the relationship between mask mandates and per-capita pediatric cases, they found “no significant relationship between mask mandates and case rates.”
The study observed over 1,800 counties from July through October 2021, which is presumed to be the largest observational sample ever conducted on the mask issue.
In fact, for most weeks, there was a non-statistically significant higher case rate among the masked counties. What this demonstrates is that with all of the CDC’s observational studies, arbitrary endpoints were clearly manipulated to show results they knew did not reflect reality.
Similarly, a study of fatality rates in 35 European countries during the 2020-2021 winter peak found no positive relationship between reduced mortality rates and mask compliance. If anything, there was a reverse correlation. “While no cause-effect conclusions could be inferred from this observational analysis, the lack of negative correlations between mask usage and COVID-19 cases and deaths suggest that the widespread use of masks at a time when an effective intervention was most needed, i.e., during the strong 2020-2021 autumn-winter peak, was not able to reduce COVID-19 transmission,” concluded the author in an April study published in Cureus. “Moreover, the moderate positive correlation between mask usage and deaths in Western Europe also suggests that the universal use of masks may have had harmful unintended consequences.”
Several months ago, an observational study published in Medicineby German doctor Zacharias Fögen compared the overall case fatality rate in 81 counties in Kansas without mask mandates compared to the 24 with mandates. He actually found a statistically significant higher fatality rate in the mask counties. “Results from this study strongly suggest that mask mandates actually caused about 1.5 times the number of deaths or ∼50% more deaths compared to no mask mandates.”
Dr. Fogen posits as a potential reason for negative efficacy that the mask-wearing can make the virions smaller and cause them to penetrate deeper into the alveoli, where they can cause pneumonia instead of bronchitis. “A rationale for the increased RR (risk ratio) by mandating masks is probably that virions that enter or those coughed out in droplets are retained in the facemask tissue, and after quick evaporation of the droplets,hypercondensed droplets or pure virions (virions not inside a droplet) are re-inhaled from a very short distance during inspiration.”
While negative efficacy is still a hypothesis, there have been documented negative side effects to mask-wearing. A preprint Italian study from earlier in May found that short-term surgical mask usage was associated with an increased inhaled CO2 level greater than 5000ppm in 90% of 10- to 18-year-olds in the sample. “Shortly after wearing surgical masks, the inhaled air CO2 approached the highest acceptable exposure threshold recommended for workers, while concerningly high concentrations were recorded in virtually all individuals when wearing FFP2 masks,” concluded the authors. “The CO2 concentration was significantly higher among minors and the subjects with high respiratory rate.”
Yet here we are, over two years into this saga, and schools are still masking children, while some that stopped are bringing back this barbaric practice. To this day, people with severe mental and physical disabilities are being forced to wear masks when seeking medical attention at health care facilities. Trauma survivors who suffer panic attacks from having their faces covered are forced to choose between panic attacks and loss of medical care.
But children will, by far, be the most harmed by this policy. The language development impediment that will result from the past two years of inhumane mask mandates is incalculable. The head of the U.K.’s Office for Standards in Education, Children’s Services and Skills found that children suffer from “limited vocabulary,” while some babies “struggled to respond to basic facial expressions,” partly due to interacting with people wearing face masks.
Talk about a cost-benefit analysis!
To this day, only a few states have banned mask mandates from coming back. The New Hampshire governor recently vetoed a bill from the state legislature banning local school boards from implementing such immoral policies upon children. What we really need is a ballot initiative in every state to spell out in the state’s constitution that a person has a fundamental right to refuse to wear a medical device and cannot be discriminated against in the realm of public accommodations for exercising that right. Moreover, there should be criminal penalties for any adult who forcibly masks a child. If we plan to wait for “the science” to catch up to reality and morality, we will be waiting a long time. It might be obvious to us that masking is cruel and ineffective, but not to the megalomaniacs in power. That power needs to be stripped permanently.
Typically, a lack of efficacy and a cataclysmic level of hundreds of different side effects would be reason to take a therapeutic off the market. But in the post-Nuremberg Code era we find ourselves in, such outcomes serve as a resume enhancer for the product. The FDA is planning a blitz of increased approvals of the shots on the youngest of Americans, yet not a single national Republican has stood up and said “No.” Only one governor, Ron DeSantis, has recommended against their use in children. Which will be the first state to block implementation of the FDA’s new therapeutic jihad on behalf of Big Pharma?
The FDA’s Vaccines and Related Biological Products Advisory Committee (VRBPAC) has an ambitious schedule for this coming June. Here are its upcoming meetings.
June 7: Approval of Novavax first time for those over 18.
June 8: Approval of Moderna in teenagers.
June 21: Approval of Moderna in kids under 6.
June 22: Approval of Pfizer in kids under 5.
June 28: Exploring new shots for new variants.
Isn’t it interesting how they are meeting about the need for new shots for the current variants after already likely approving old shots on babies who don’t need the shots and for a variant that hasn’t existed for over a year?
Here we have many European countries banning the Moderna shot on those under 30 because of myocarditis, yet our government will likely expand its use to babies at a whopping dose of 25 micrograms! We now have over 1.2 million adverse events reported to VAERS, and CDC researchers admitted in a JAMA paper that the myocarditis numbers – just shy of 40,000 – are “likely” underreported. Also, we now know that Pfizer and the FDA knew about 1,223 deaths shortly after release. As for Moderna, we don’t have a single court-released document from the company yet, so who knows what they are hiding?
It would be one thing to approve something that worked amazingly for COVID despite terrible side effects. But the shot is a complete bust.
The expectation of negative efficacy from these shots has become so widely accepted that now the only question is who is the next famous politician or celebrity to get COVID multiple times after having gotten three or four shots. Take a look at this chart from the Walgreens COVID-19 index of all its testing this past week broken down by vaccination status:
Have you ever seen a vaccine of which the more doses you get, the more likely you are to test positive? Notice how the unvaccinated account for a lesser share of cases than either their share of the population or of Walgreens-administered COVID tests. The results are based on 81,818 tests administered nationwide in Walgreens stores from May 2 through May 8.
So now they want to take vaccines with such counterproductive outcomes and foist them upon children? Remember, the FDA has already demanded the manufacturers produce a study on subclinical myocarditis. In its Pharmacovigilance Plan Review Addendum for Comirnaty, the agency cited one study at the time of Pfizer’s approval noting that subclinical myocarditis might be 60 times as prevalent as clinical myocarditis. That would bring down the 1 in 1,000 rate among young males to as low as 1 in 17 for subclinical ticking time bombs!
Let’s not forget that in all the children’s trials, there were zero deaths and hospitalizations in the placebo groups. So, what exactly were we trying to protect against – even before we knew the shots weren’t effective and possibly negatively effective? Cold or flu-like symptoms? Well, here is the data of side effects from Moderna’s 5-11 trial:
“The most frequently reported adverse reactions were pain at the injection site (92%), fatigue (70%), headache (64.7%), myalgia (61.5%), arthralgia (46.4%), chills (45.4%), nausea/vomiting (23%), axillary swelling/tenderness (19.8%), fever (15.5%), injection site swelling (14.7%) and redness (10%).”
So even before we get to more serious side effects like heart inflammation, we have a massive percentage of children getting flu-like symptoms from the shots, which is what they would get anyway from the virus. How can this pass the threshold of any principle laid out in the Nuremberg Code or the Helsinki Declaration?
It’s gotten so bad that Pfizer and Moderna can no longer rely upon dubious trials showing a 90% reduction in COVID. Especially for young children, even for mild infection, they couldn’t even manipulate any data showing any degree of efficacy, so they had to rely on an arbitrary measure of antibody titers rather than clinical outcomes. In shocking statement before the House Select Subcommittee on the Coronavirus Crisis, Peter Marks, director of the FDA’s Center for Biologics Evaluation and Research, conceded they would approve the shots on young children even if the manufacturer’s own dubious data shows less than 50% efficacy (and even that is only for minor illness).
“If these vaccines seem to be mirroring efficacy in adults and just seem to be less effective against Omicron like they are for adults, we will probably still authorize” because they nonetheless reduce the risk of severe disease in the mildest COVID variant, Marks revealed during the May 9 briefing.
Just keep in mind that, according to the CDC, 74.2% of kids 0-11 already got natural immunity from prior infection. So not only will they fail to test kids for antibodies before injecting them, but even the remaining quarter who might be COVID-naive, they are trading risk of death and severe side effects (and pervasive mild side effects) for a possible tiny degree of very short-term efficacy against sniffles, but a long-term negative efficacy against those sniffles. A preprint study by the NY State Department of Health in February showed that the Pfizer shot was just 12% effective against the first Omicron variant for 5- to 11-year-olds, but drops to -41% after just 42 days!
How can any of these shots be administered until we understand why so many data points seem to show intensifying negative efficacy with time? It’s like investing in a stock that first goes up for a few weeks, but then you erase all the gains within a few days and then gradually lose all your principal investment. Every Republican claims to be pro-life, but distributing these shots to young children is not pro-life, even if they are not quite mandated. Would they sit idly by if the federal government distributed abortifacients throughout their states?
For all the talk about Putin’s authoritarian grip over former Soviet states, we have our own authoritarian Putins now governing Western democracies and crushing all political dissent. Holding someone without bail for organizing a peaceful protest against the government sounds like something Putin would do, yet it is now happening in Canada and has already been happening here against those who did not engage in violence on Jan. 6. Meanwhile, these same Western leaders support de-incarceration for the most violent criminals, demonstrating that it’s not even about authoritarianism, but a two-tiered society built upon the ideals of fascism.
Last Thursday, Tamara Lich, one of the organizers of the trucker convoy who set up the original GoFundMe account, was arrested in Ottawa for simply opposing the Trudeau regime and organizing a peaceful protest. Not a single person from the hundreds of thousands of truckers acted violently, a few blocked roads, and Lich herself did nothing. She is being charged with “counselling to commit mischief,” which reeks of Iranian-style prosecution.
On Tuesday morning, Ontario judge Justice Julie Bourgeois denied Lich the opportunity to post any bail, even though she promised not to engage in more lawful protests and instead return to her home in Alberta. “I cannot be reassured that if I release you into the community that you will not reoffend,” Bourgeois said. “Your detention is necessary for the protection and safety of the public.”
Those who follow my running column on robbers and gun felons who get released without bail, and even some murderers who get released on low bail despite massive criminal records, can appreciate the rich irony. Lich might reoffend by committing an action that is not only legal but serves as the cornerstone value of dissent in a free and democratic society. If this standard were applied to BLM, there would literally be millions in jail today, and they often engaged in violence, not to mention more widespread blocking of roads.
Justice Bourgeois is a former liberal candidate for parliament and was endorsed by Trudeau in 2009. Thus, we are now at a point in Western (former) democracies when political prisoners cannot get a fair trial because the courts are completely co-opted by regime-supporting judges. Worse, Bourgeois once excused rising violent crime as “desperate people going through desperate times and using desperate measures.”
Hence, the very same judges and politicians who believe that political dissent is a dangerous crime also believe that career violent criminals need to be let out of jail. The same people who want to deny peaceful citizens the right to carry a gun seek to release every gun felon who has committed violence with a gun.
To that end, what is happening in Western countries is even worse than China or a return to pre-enlightenment Western governing values. In China, they wouldn’t tolerate murderers and carjackers. They will at least apply their harshness with equality – to an extent. What we are seeing in Canada and the U.S. is a form of postmodern Western-style fascism that elevates criminal behavior to the highest ideals of society while punishing the expression or utilization of basic human rights if they violate those ideals.
This is the plain definition of fascism. It doesn’t have to always be rooted in race. Merriam-Webster defines fascism as “a political philosophy, movement, or regime (such as that of the Fascisti) that exalts nation and often race above the individual and that stands for a centralized autocratic government headed by a dictatorial leader, severe economic and social regimentation, and forcible suppression of opposition.” This is what we are seeing in Western countries today. It’s not a matter of targeting any one race but creating a standard of national interests and announcing that anyone who doesn’t subscribe to those interests – even if they affect one’s body in the most intimate way – is a threat to the nation and needs to be segregated, discriminated against, persecuted, and suppressed.
It’s not about equal-opportunity authoritarianism, because it is directed solely at those who don’t fit the national standards. Thus, we are witnessing the worst influx of illegal immigration and domestic crime precisely during the time of the most heavy-handed authoritarianism against “some” citizens. At the same time that we have the most autocratic stay-at-home order of all time, we experienced the greatest ubiquitous mass gatherings in history through BLM protests and riots.
It’s easy to rest on our laurels and thank God we are living south of the 50th parallel, but we have already seen political dissidents held without bail for a year with no criminal record for very nebulous charges that are clearly directed at chilling political dissent, not deterring violent or even disruptive behavior. For example, Couy Griffin, a county commissioner in New Mexico and founder of Cowboys for Trump who certainly had no prior criminal record, was initially held without bail for several weeks, despite never having stepped foot in the Capitol or committed assault or vandalism. The unappointed magistrate judge kept him solely because of his political views and used that as pretext to show he is a flight risk.
“I don’t think that the defendant will follow my conditions if he believes I am part of this machine of the democratic process,”proclaimed magistrate Judge Zia Faruqui at a hearing on Feb. 1, 2021. She went on to note that his political views, because she disagrees with them, makes him eligible to be held without bail – something not done for many murderers with massive rap sheets. She said that believing the election was stolen was “no different than people not believing facts or science.” No wonder they now want to criminalize dissent from their illogical and unscientific “public health” ScIeNcE.
It is therefore clear that we already have Canada’s problem of the judicial system criminalizing political opposition and thought crimes. Yet this is occurring at a time when our judicial system has largely done away with pretrial holding even for violent repeat offenders. Here are just a few recent stories to consider when trying to process the breathtaking speed at which we have devolved into an authoritarian state … except for what actually needs deterrent from strong authority!
James Tubbs, 26, who plead guilty to molesting a child at a Los Angeles Denny’s restaurant restroom, will serve no time in prison and will not have to register as a sex offender, thanks to the new rules put in place by prosecutor George Gascon. Tubbs, who now believes he is really a woman, is instead being held in a female juvenile facility, even though he is an adult male, because he was just shy of his 18th birthday when he committed the crime. Fox News recently released a tape of Tubbs bragging about beating the system. “I’m gonna plead out to it, plead guilty,” Tubbs says in one recording. “They’re gonna stick me on probation, and it’s gonna be dropped, it’s gonna be done, I won’t have to register, won’t have to do nothing.”
There is a carjacking epidemic in almost every major city. Recently, Chicago police superintendent David Brown revealed that 60% of all incidents were perpetrated by juveniles and that the system offers no real consequences for them.
Speaking of political crimes, how about attempting to assassinate a mayoral candidate? Well, in our fascist social “equity” system, it depends on the race and motive of the perpetrator. Earlier this month, BLM activist Quintez Brown was charged with attempted murder for stepping into the campaign headquarters of Louisville mayoral candidate Craig Greenberg and opening fire. Luckily, the bullets only grazed the candidate’s clothing and the shooter was stopped and apprehended. He came with extended magazines and clearly was coming as an assassin, but a judge let him out on $100,000 bail, which was posted by national BLM umbrella groups. “There is simply no defense for a would-be assassin to be released on bail, 60 hours after firing on his intended target,” Adam Edelen, the former chief of staff for former Democrat Kentucky Governor Steve Beshear, tweeted. Can you imagine if someone from the trucker movement had done this to a prominent pro-mandate politician?
Bronx Supreme Court Justice Naita Semaj-Williams just allowed two teenagers charged with murder, manslaughter, robbery, gang assault, and other crimes to be released without posting bail. In a previous case earlier this month, Semaj-Williams walked back a $60,000 bond for a criminal charged with attempted murder and released him on his own recognizance.
These situations are occurring even in Texas. In 2019, Treveon Tatum, 20, was charged with murder but released by a Houston judge on just $50,000 bond. Despite being arrested again the following April for felony aggravated assault with a deadly weapon, Tatum still did not have his bail revoked. Despite violating the terms of his bail multiple times, he was never re-incarcerated. Then, on Feb. 8, he was charged again with a new murder.
While COVID is being used an excuse to jail business owners and political dissidents, the same virus is being used as pretext to release true public safety threats. Earlier this month, Garrett W. Caspino was cited twice by police for criminal trespassing while acting erratically in a residential neighborhood of Corvallis, Oregon. However, he wasn’t arrested “because of COVID-19 protocols.” But just an hour later, he allegedly broke into a home in broad daylight, pulled down his pants, and choked the female homeowner against the wall while showering. He was later chased out of the house by the victim’s boyfriend. Despite the seriousness of the charges and the clear likelihood he will “reoffend,” Caspino will still have an opportunity to post bail, albeit a high amount.
The raison d’etre of the existence of Western governments is plainly spelled out in the preamble of our Constitution – to “establish Justice, insure domestic Tranquility, provide for the common defense, promote the general Welfare, and secure the Blessings of Liberty to ourselves and our Posterity.” Yet we now have a government that ensures tyranny and promotes the curse of violent anarchy while perverting justice based on politics and identity. One could not possibly abrogate the underpinnings of our social contract in a more grotesque manner than what today’s global elites governing Western countries are doing. This is unsustainable and must change. It is our right – our duty – to demand a new government “to provide new Guards for their future security.” The same failed political strategies of the past do not speak to the magnitude of corruption in our government.
If the truth hurts your narrative, you must censor it. But what if your own information harms your own narrative? Well, then you stop publishing it. For the past few months, Scotland has been publishing age-stratified case rates by vaccination status in a very well broken-down chart every Wednesday afternoon, similar to the way the U.K. published the data every Thursday. The common thread observed from these trends was that the unvaccinated had the lowest case rate, the double-vaccinated had even higher death and hospitalization rates, and the triple-jabbed gradually had increasingly higher case rates, which clearly doesn’t portend good news even for hospitalization and death in the long run. When people like me started using their data, we were lambasted by the “fact-checkers” paid for by Big Pharma. Now Scottish health officials announced they will not be publishing the data at all.
“Public Health Scotland will stop publishing data on covid deaths and hospitalisations by vaccination status — over concerns it is misrepresented by anti-vaxx campaigners,”reports the Glasgow Times.
The notice of change was published on page 29 of the latest, and evidently final, Wednesday report from Feb. 16. “PHS is aware of inappropriate use and misinterpretation of the data when taken in isolation without fully understanding the limitations described below,” they decried.
You mean like screenshotting their own charts?
Obviously, there can be confounding factors, but those factors actually cut both ways. However, at the end of the day, these are age-stratified adjusted case rates per 100,000 and are completely fair game to use. No vaccine that is anywhere near as effective as they make it out to be should be netting these results.
Here is the latest case rate chart from the final report:
As you can see, for the past two weeks they have been placing disclaimers at the bottom of the charts.
What the chart clearly shows is what we have been seeing throughout the world — from the U.K., Canada, and Israel, for example — namely, that the second shot has gone negative a long time ago and the third shot is gradually following in the same direction. The public health officials themselves are demanding that people get boosters because they say the other shots wane. Well, logic would dictate that now that we are three to five months into the boosters in most places, they are waning as well. We also know that waning efficacy is potentially associated with a Trojan horse effect of antibody dependent disease enhancement, something the FDA admitted was never studied in the long run (at the time they thought the shots wouldn’t wane) but would be a risk “potentially associated with waning immunity.”
The main argument of those who are against us screenshotting their own charts to point out what they themselves have admitted is a speculative theory that perhaps the vaccinated test more often than the unvaccinated. That is a purely speculative confounding factor in the favor of the vaccine, but here is a concrete proven confounder against the vaccine: Scotland counts the first 21 days of the first vaccine as unvaccinated and the first 14 days of the third vaccine as double-vaccinated. We already know from Alberta’s data (which of course they also took down since we cited it) that roughly 40% of cases, 47.6% of hospitalizations, and 56% of deaths among the vaccinated occurred within 14 days of vaccination! So if anything, many of the cases and deaths ascribed to the unvaccinated are caused by the immune suppression of the first shot, and many cases and deaths ascribed to the double-vaccinated makes that cohort look even worse than it already is in order to ameliorate the image of the boosters.
Furthermore, if the higher case rates among the vaccinated are the result of a higher testing rate, then why would the double-vaxxed also be worse off than the unvaccinated for hospitalizations and deaths, as PHS has been showing for weeks in its other charts?
It’s quite evident that everyone is tested in the hospital. If anything, it stands to reason that the unvaccinated would be more aggressively tested even when admitted for other ailments and therefore potentially be roped into incidental hospitalization counts more often than the vaccinated. For example, in June 2021, Scripps Health in San Diego announced it would only test unvaccinated asymptomatic patients but not the vaccinated. Clearly, the testing requirements of the unvaccinated and the counting of the (immune-suppressed) partially vaccinated as unvaccinated would be confounding factors for woefully overestimatingunvaccinated hospitalizations, not the other way around.
Also, why would the triple-vaxxed test less often than the double, who test more often than the single or unvaccinated? And why would the waning always continue in the same direction throughout the pandemic? As you can see from the U.K. Health Security Agency weekly reports, the efficacy of the shots constantly wanes with every new weekly report, a phenomenon that cannot be explained away by testing rates.
2.17.22: UK infection rates, since Omicron arrived, rose much faster among the boosted vs the unvaxxed & remain higher in all boosted adult cohorts. Both boosted & unvaxxed continue to get infected & spread – and in adults, the boosted much more so – invalidating vaxx mandates. pic.twitter.com/cpDsOkcuSb
Clearly, this picture points to dangerous waning efficacy that plagues every cohort within a few months.
The bottom line is that during the final week of reporting in Scotland, just 12% of the deaths are among the unvaccinated, and that is including the 21-day grace period of counting the single-jabbed as unvaccinated. Nobody is suggesting that there is no efficacy for some people for a period of time against serious illness before the shots wane. But to suggest that this is a pandemic of the unvaccinated, to ignore the negative efficacy on infection which has been true across the board since last summer, and to obfuscate the concern of waning efficacy on critical illness even as they themselves demand boosters defies willing suspension of disbelief.
Unbelievably, PHS admits that the shots first suppress the immune system before they ramp up antibodies. But instead of using this as a strike against the shots, they use that is a strike against the unvaccinated and assert that it is a factor for why you can’t even compare hospitalization or death rates. “Individuals who have not completed their vaccine schedule may be more susceptible to a severe outcome and could result in higher COVID-19 case, hospitalization and death rates in the first and second dose vaccine groups,” claims PHS in the report.
But if that is true, that is the fault of the manufacturers who made a shot that first makes you vulnerable during an ongoing pandemic. It’s one thing to have a shot that makes you more vulnerable for a few weeks during the off-season of a virus. But to do so during the pandemic is akin to telling someone in a foxhole during a firefight that they will be safer in a bunker 100 yards ahead but must first run across the field to get there. The risk of making that run should be counted against the bunker option, not the foxhole.
In other words, as I wrote in my original piece on the Scottish data that was “fact-checked,” “You have to look in totality where we are headed rather than manipulating a snapshot of time.” You can’t just pull out one period of time of some efficacy for some people. You need to consider the following:
Vaccine injuries short term and long term, known and unknown;
Other safer treatment options for COVID itself;
A leaky vaccine that wanes in efficacy and runs the risk of enhancing the virus itself even while offering temporary protection for some;
The cost to the immune system of constantly boosting people to deal with the abovementioned concern of waning efficacy and enhancement.
The bottom line is that the social media guardians are looking at a snapshot of time. If they were to study the trajectory and progression of the virus and the vaccine throughout the year, they would recognize an unmistakable pattern of waning and then negative immunity. A large study published in the New England Journal of Medicine by Weil Cornell Medicine-Qatar found (table 3) that the Pfizer vaccine waned very quickly after four months. By seven months, when adjusted for those in Qatar who already had prior infection, the Pfizer shot was -4% effective against transmission and just 44.1% effective against severe illness. Also, effectiveness against asymptomatic infection was -33% after seven months.
A Swedish preprint study in October 2021 looked at 1.6 million people in Sweden to examine infection rates and critical illness rates by vaccination status. They found a sliding scale of efficacy that wanes with time, but eventually turns negative. Here is a presentation of fully adjusted vaccine effectiveness against symptomatic infection for various demographics after 210 days:
Clearly, it was known early on that the vaccine wanes and has the potential to go negative even with Delta, for which both natural infection and the vaccines offered better immunity. It stands to reason that this is certainly the case with Omicron, making it abundantly clear that the negative efficacy rate has more to do with potential Trojan horse antibodies than it does with vaccination-status bias of testing rates.
So what’s the solution? Go for a fourth and fifth shot? This week, Israeli researchers published a preprint study on the efficacy of the fourth shot, which found that after just one month, Pfizer’s shot is down to 30% efficacy and Moderna is down to 11%. At the same time, “Local and systemic adverse reactions were reported in 80% and 40%, respectively.” They conclude, “Low efficacy in preventing mild or asymptomatic Omicron infections and the infectious potential of breakthrough cases raise the urgency of next generation vaccine development.”
Remember, the FDA’s industry guidance for EUA status (p. 13) requires a 50% threshold of efficacy to even get emergency use authorization, much less full approval!
Thus, who is actually misreading or inappropriately using data here?
The Israeli study also concluded that “most of these infected HCW [health care workers] were potentially infectious, with relatively high viral loads. Thus, the major objective for vaccinating HCW was not achieved.” Full stop. The biggest public policy debate is over the fact that somehow you not getting the shot affects other people. Here we see that even people with four shots were still infectious with high viral loads. To what degree the shot offers some degree of protection from serious illness for some people for some period of time should be a decision left to the people. Perhaps other people would like to choose therapeutics that offer protection that don’t run the risk of severe adverse reactions. But none of that should have bearings on another human being, and none of that should justify human rights violations. This entire saga began with censorship of the work of others because the narrative assertions could not withstand peer review. Now we’ve come full-circle, in which the governments’ own data must be censored because the narrative assertions cannot withstand the scrutiny of their own data.
It’s utterly senseless. Pfizer is now asking to authorize a dangerous, outdated shot for babies and toddlers, for whom the virus does not pose a statistical risk and for a virus against which the shots have failed to show any benefit. Yet, just as taxes and death are a certainty in life, you can bank on the FDA never turning down any Pfizer request. This is where Republican governors must serve as the safety net for the people. They must actively oppose expanding the shots to the final control group against the greatest experiment on mankind.
In one of the most shocking and immoral moves since the beginning of the pandemic, Pfizer is submitting its request this week for emergency use authorization of its COVID shot for babies as young as 6 months old through 5 years old. They are quite literally pushing a shot with the hopes of ameliorating symptoms (not stopping transmission) of a virus that is a cold for young children and much less dangerous than RSV. But here’s the kicker: The trial they conducted showed that two doses failed to even produce positive results, and they are still working on a trial for a three-dose regimen. Plus, we have a new variant. So, what exactly are they seeking authorization for?
As other countries are already recommending against vaccinating those under 12, our government will likely approve this shot for babies and young children based on a failed trial. There was never any efficacy in the shot because no child in the trial got seriously ill to begin with. So, they chose a trial endpoint around levels of antibody titers. Putting aside for a moment the premise that higher antibody titers (as opposed to T cells) are necessarily a good thing and won’t cause original antigenic sin, their own trial failed to achieve these endpoints in 2- to 4-year-olds. Which is why Pfizer announced in December that it was beginning a trial on a three-dose regimen. So how can they seek authorization of the failed two-dose trial for what is essentially a new virus?
One of the precepts of the Nuremberg Code: “The degree of risk to be taken should never exceed that determined by the humanitarian importance of the problem to be solved by the experiment.” There is no way pursuit of an already flawed vaccine can be justified on young children, even if it still had a degree of efficacy and wasn’t outdated. A recent study from the U.K. showed that even immunocompromised children were not at an elevated risk for severe COVID. The study of 1,527 immunocompromised children and young adults found “no increased risk of severe SARS-CoV-2 infection.” None of those even more vulnerable children died.
While there likely have been a tiny number of severely ill children who have died of the virus, it’s extremely hard to tell how many of the recorded deaths were legitimately caused by the virus itself. A large COVID study conducted in Germany found just three pediatric COVID deaths out of a million. The same analyst found zero deaths occurred in children under 5.
Already among older children, no positive benefit was found in the vaccine, even when the vaccine was working better. An Israeli study published in the New England Journal of Medicine found ZERO deaths or severe illnesses BOTH in the vaccinated and in the control (unvaccinated) groups of 12- to 18-year-olds in a 29-day follow-up of their vaccination. Under what pretext could the government possibly justify COVID as an emergency in this age group, and based on what evidence does this vaccine address that “emergency?”
On the flip side, the CDC, in a study in published in JAMA just conceded that the VAERS data on myocarditis was indeed an accurate reflection of an increased risk of heart inflammation following the vaccines. “Based on passive surveillance reporting in the US, the risk of myocarditis after receiving mRNA-based COVID-19 vaccines was increased across multiple age and sex strata and was highest after the second vaccination dose in adolescent males and young men,” concluded the CDC researchers. “This risk should be considered in the context of the benefits of COVID-19 vaccination.”
More broadly, over 22,600 vaccine deaths and over 1 million injuries have been reported to VAERS. We already know from previous studies that VAERS only captures 1% of adverse events, and no other shot has come with such a stigma against reporting it for harm, often at the threat of the physician losing his job. Medicare data seems to hint at a much broader cohort of vaccine casualties. The military’s epidemiological database also seems to indicate a very disturbing trend of neurological and cardiological disorders rising in association with the take-up of the vaccine.
How can this be foisted upon the youngest children — with no apparent benefit — when they concede, “Long-term outcome data are not yet available for COVID-19 vaccine–associated myocarditis cases”?
There are no long-term cancer studies, there are no long-term studies on what this does to one’s immune system, and there are no long-term studies on autoimmune diseases, even though the VAERS data and the Pfizer surveillance data from early 2021 raises some concerns. Plus the vaccine is for a virus that is not a threat to children.
Think about it: Monoclonal antibodies can get their existing EUA pulled based on the arrival of a new variant, yet shots that have already proven to be outdated – and are associated with greater infection rates – can secure official full approval and then EUA for babies with a new variant that was never run through a clinical trial.
As such, for a governors to merely take a neutral stance while allowing this travesty to plague the children of their states is unacceptable. Governors have a responsibility to direct their respective health departments to conduct the proper oversight that the FDA has abdicated and demand a moratorium on shots for children until a proper cost-benefit analysis can be conducted. At a minimum, they should join together in a lawsuit to enjoin the EUA because Pfizer has failed to prove the shots meet the eligibility thresholds in the EUA statute.
Moreover, Republican governors and legislators have an obligation to treat Pfizer like Planned Parenthood and cut all political ties with the company’s lobbying groups. Bio-medical fascism and the breach of informed consent is a greater pro-life cause than opposition to abortion right now, because its practitioners are encouraging all children to get something with only a potential downside. It is the equivalent of forcing abortions upon us, not just permitting them.
The final precept of the Nuremberg Code reads as follows: “During the course of the experiment the scientist in charge must be prepared to terminate the experiment at any stage, if he has probable cause to believe, in the exercise of the good faith, superior skill and careful judgment required of him that a continuation of the experiment is likely to result in injury, disability, or death to the experimental subject.” If after everything we have learned, they won’t even discontinue this experiment on babies, then we truly have learned nothing since that dark era of history.
Were the cloth masks just for psychological training purposes to get us to the main course of obsequious servitude to the gods of Fauci?
It took nearly two years, but the “public health experts” are finally admitting what industrial hygienists knew from day one: Masks do not work against airborne viruses. Yet rather than immediately remove these draconian restrictions – including masking 2-year-olds on airplanes and schoolchildren for hours on end in many states – they are seamlessly gliding into the new position of promoting N95 respirators. Following the inveterate patterns of the past two years, they use the failure of their first position to their advantage to further panic people into blindly following their next recommendation … until that becomes a mandate as well.
On Jan. 2, former FDA administrator Scott Gottlieb, the media’s go-to “expert” on all things pandemic, admitted what we all knew since 2020 but that got us banned from social media for saying so. “Cloth masks aren’t going to provide a lot of protection, that’s the bottom line,” said Gottlieb on Meet the Press. “This is an airborne illness. We now understand that, and a cloth mask is not going to protect you from a virus that spreads through airborne transmission.”
Two days later, the New York Times ran an article telling people where to get N95s, states began mailing out N95 variations, and the CDC put out a new message, which between the lines, gives the impression that if you are not wearing an N95, you don’t really have protection. The Biden administration plans to distribute millions of them to local pharmacies. But is there really any evidence that the same people who were wrong about masks are now suddenly connected to God’s word when it comes to respirators? And who says it is safe for people to wear something like that for long periods of time, which until now required rigorous testing, medical exams, and training?
Yes, N95s, unlike masks, actually meet the standard for PPE in hazardous environments. But for which sort of hazard? Not an airborne respiratory virus. Stephen Petty, a certified industrial hygienist and hazardous exposure expert, sent me a copy of an N95 usage label made by 3M that he enlarged into an infographic. It turns out the company’s own disclosure blows up the myth of using an N95 for viral protection.
The label confirms what everyone understood prior to the mask mania of COVID: Neither masks nor N95 respirators can stop aerosols, certainly not viral ones, which are much smaller than bacteria. What’s truly revealing is that the label recommends against relying on them for source protection even against asbestos particles, which are on average 5 microns – 50 times larger than SARS-CoV-2 virions.
A large randomized controlled trial published just months before the discovery of SARS-CoV-2 — before masking became a political and social control tool — showed no benefit to N95s over surgical masks in terms of protection against the flu. “Among outpatient health care personnel, N95 respirators vs medical masks as worn by participants in this trial resulted in no significant difference in the incidence of laboratory-confirmed influenza,” concluded the authors of the large trial, published in JAMA on Sept. 3, 2019.
Also, remember, that most people are not wearing sealed N95s. They wear the respirators loosely on their faces as they do surgical masks. Also, many of them are the Chinese version KN95s. Even the CDC admits, “About 60% of KN95 respirators NIOSH evaluated during the COVID-19 pandemic in 2020 and 2021 did not meet the requirements that they intended to meet.”
The same study (Shah et.al.) that found just 10% and 12% reduction in aerosols for cloth and blue surgical masks respectively, actually found that KN95s worn improperly with 3mm gaps between the face and the respirator, as most people wear them, only offer 3.4% filtration efficiency – less than the cloth masks.
And remember, these studies are all conducted in labs, not in the real world, where no study has shown a statistically significant benefit to masks, and the basic epidemiological data has disproven the efficacy for two years.
Take Austria, for example, where they have been mandating N95 respirators in stores. Can you spot the efficacy?
The notion that children can properly wear a form-fitted N95 that effectively seals is both absurd and dangerous. And anything else will absolutely not work. There’s clearly an inverse relationship between safety and efficacy. The only thing that might possibly work will cause danger, which is why the federal government has long mandated very specific criteria for wearing respirators.
“While some misrepresent N95s as masks, they are actually respirators and will require one to follow the OSHA requirements for respirators under the Respiratory Protection Standard (RPS) 29 CFR 1910.134 (e.g., written program, medical clearance, initial fit testing, annual fit testing, no facial hair, worker training),” said Petty in an interview with TheBlaze. Stephen Petty has served as an expert witness in hundreds of industrial hazardous exposure court cases and now serves as a witness for those bringing lawsuits against irresponsible mask mandates. Here is a list of OSHA requirements, per Petty’s presentation, that would have to be met for usage of N95 respirators:
There’s a good reason why these requirements were put in place by OSHA. To the extent one actually properly seals an N95 respirator to the face (which few will do), it causes significant medical concerns. Here are some findings from an extremely exhaustive qualitative and substantive evaluation of 65 mask studies by German researchers:
In nine of the 11 scientific papers (82%), we found a combined onset of N95 respiratory protection and carbon dioxide rise when wearing a mask. We found a similar result for the decrease in oxygen saturation and respiratory impairment with synchronous evidence in six of the nine relevant studies (67%). N95 masks were associated with headaches in six of the 10 studies (60%). For oxygen deprivation under N95 respiratory protectors, we found a common occurrence in eight of 11 primary studies (72%).
Thus, to the extent anyone could achieve a meaningful degree of efficacy against virus particles with a respirator – something yet to be proven – it will come at a terrible cost. Even with regular masks, before our public health officials lost their minds (and hearts), it was understood that they are not harm-free. Here is a write-up from the Missoula, Montana, city health department recommending against the use of masks during wildfire season in Montana:
Masks are uncomfortable (they are more comfortable when they are leaky – but then they do not provide protection). They increase resistance to airflow. This may make breathing more difficult and lead to physiological stress, such as increased respiratory and heart rates. Masks can also contribute to heat stress. Because of this, mask use by those with cardiac and respiratory diseases can be dangerous, and should only be done under a doctor’s supervision. Even healthy adults may find that the increased effort required for breathing makes it uncomfortable to wear a mask for more than short periods of time. Breathing resistance increases with respirator efficiency.
The Montana Department of Health emphatically writes in bolded letters that N95s that seal are the only things that might help against smoke particles (which are around 1 micron, 10 times larger than most viral virions), but warns of health risks. “Note that respirator masks should be a last resort, as they are difficult to fit correctly, decrease oxygen intake, are hot, and can easily leak when worn improperly.” They go on to add, “People who are not physically fit may experience difficulty going about daily tasks due to reduced oxygen intake. It is more important to have enough oxygen than to have clean air – if you are using a respirator and feel faint, nauseous, or have trouble breathing, take the mask off.”
On the Washington Department of Health’s website guidance for wildfires, it is made clear that “masks are not approved for children” and that “it is harder to breathe through a mask, so take breaks often if you work outside.” The Sacramento County Department of Health Services states, “N95 respirator can make it more difficult for the wearer to breathe due to carbon dioxide buildup, which reduces the intake of oxygen, increased breathing rates, and heart rates.”
Just a year ago, CDC Director Rochelle Walensky swatted down the idea of wearing N95s. “They’re very hard to breathe in when you wear them properly,” Walensky said. “They’re very hard to tolerate when you wear them for long periods of time.”
Thus, whether we are talking about masks or N95s, it’s quite evident that they are either unsafe or ineffective. They can often be both unsafe and ineffective, but they can never be effective without being unsafe, unless worn by the right person with the right training in limited environments for short periods of time.
And this is just the scope of physical harm. One speech therapist in Palm Beach County is seeing a 364% increase in referrals from pediatricians for babies and toddlers with speech delays. “It’s very important that kids do see your face to learn, so they’re watching your mouth,” said a clinic director and speech-language pathologist at the Speech and Learning Institute in North Palm Beach.
How our governments can mandate something this immoral and illogical on our bodies indefinitely without due process, evidentiary standards, or a constitutional interest balancing test is astounding. Every state needs a constitutional amendment explicitly banning this from ever happening again. Biden promised 100 days of mask-wearing, but we are now approaching a full year without any end in sight.Just remember, if a government can criminalize our breathing without due process, what can it not do to us without recourse?
One of the most durable public health trajectories over the past 50 years has been the consistent decline in infant mortality in countries with first-world health care. Yet in September, Scotland experienced such a spike at least in neonatal deaths that it rivaled levels not seen since the 1980s. What on earth would cause such a sudden bizarre spike? Nobody seems to have the answer — nor do they want to study all of the potential culprits.
In September, Public Health Scotland announced that 21 newborns had died that month, triggering an investigation because the numbers rose above an upper control limit for the first time in four years. According to the Herald Scotland, “the figure for September – at 4.9 per 1000 live births – is on a par with levels that were last typically seen in the late 1980s.”
As you can see from the Public Health Scotland (PHS) data, the upper control limit was breached in September, which PHS believes “indicates there is a higher likelihood that there are factors beyond random variation that may have contributed to the number of deaths that occurred.” After all, the five-year average appears to be about 2.2 per 1,000 live births, so September’s numbers are more than double the average.
Although the incidents of neonatal death tend to fluctuate every other month, the levels appear to be elevated, on average, without the usual intermittent dips below the baseline throughout the entire year of 2021. This is astounding given how much the general trend of infant mortality has declined since the 1980s.
Based on media reports, it appears that the entirety of the public health investigation revolved around whether COVID itself was the culprit of the unusual number of neonatal deaths. The problem is that we didn’t see any of this death in the first year of the pandemic. Also, it was only infants who seemed to experience a sharp increase in death, the least likely cohort to be affected by the pandemic.
In December, PHS announced that based on preliminary findings, it has no evidence that COVID was the culprit. “There is no information at this stage to suggest that any of the neonatal deaths in September 2021 were due to Covid-19 infection of the baby,” said PHS, according to the BBC. “Likewise, preliminary review does not indicate that maternal Covid-19 infection played a role in these events.”
Well, that’s pretty obvious, but what is the culprit for such an unusual trend?
“Preliminary information on prematurity suggests that the number of babies born at less than 32 weeks gestation in September 2021 was at the upper end of monthly numbers seen in 2021 to date. This may contribute to the neonatal mortality rate, as prematurity is associated with an increased risk of neonatal death.”
But why would that cause neonatal deaths not seen since the 1980s, and why would there be more prematurely born babies?
With so many other vaccine safety signals being seen, there is no desire to even look at the possibility that an experimental shot that was not studied in pregnant women – yet was widely distributed to them – had something to do with it. We have no idea what caused this spike, but here’s why any logical person would commence an inquiry around the shots.
The shots were not studied in pregnant women, and it’s not like we haven’t seen other problems. There are over 21,000 deaths in VAERS and over 1 million adverse events, including tens of thousands of reproductive-related incidents.
We know that this shot has caused menstrual irregularities like we’ve never seen before. A University of Chicago survey sought to recruit 500 women with menstrual irregularities in order to study the cause and effect, and instead, researchers got 140,000 submissions. One study found that 42% of women experienced heavier bleeding, while only 44% reported no changes to their menstrual cycles. A whopping 66% of post-menopausal women experienced breakthrough bleeding. This all goes to show how the 20,000 menstrual irregularities reported in VAERS are a joke because the system only captures a fraction of the adverse events.
As of Dec. 31, there were 3,511 miscarriages reported to VAERS. Remember, this is something that is extremely hard to pin on the vaccine, so the fact that so many felt they could report it demonstrates there is likely a woeful underreporting rate. Here is the presentation from Open VAERS, which shows the number of reported miscarriages peaking around August/September in the United States.
Does any of this mean we can conclusively say the shots are causing reproductive issues? No. But there certainly are a lot of safety signals that should be followed up on rather than dismissed. I asked Dr. James Thorp, a Florida-based OB/GYN and maternal-fetal medicine specialist with over 42 years of experience, if he was concerned about these signals. “To the extent of a broad statement that menstrual irregularities are usually minor issues is a true statement,” he said. “However, in the context of the massive increase in menstrual irregularities associated with the vaccine, there are very serious potential implications. It supports the cumulative evidence that the jabs’ lipid nanoparticles concentrate in the ovaries and affect/infect/expose ALL ovum to the LNP and cargo mRNA [and] is extremely serious.”
Thorp notes that the LNPs can be inflammatory and they likely penetrate every area of the body and, by extension, the fetus. “The lipid nanoparticles (LNPs) easily pass through all the natural barriers that God created in the human body. LNPs are extremely small spherical particles with an outer lipophilic (fat-soluble) membrane containing the mRNA cargo. There may be billions of LNPs in the COVID-19 jab that do not remain in the deltoid muscle; they are readily dispersed throughout ALL bodily tissues, easily pass through the maternal blood-brain barrier, the placental barrier, and the fetal blood-brain barrier.”
Thorp observes that whereas men continuously make more sperm throughout their lives, women have a finite number of eggs, which means that “every single one is exposed to the LNPs for life.”
Previous studies have shown nanoparticles to be a source of fetal inflammation. “Nobody knows the potentially catastrophic results of this,” warns Thorp. “In my area of expertise of maternal-fetal medicine, we have researched for decades on the catastrophic effect of inflammatory processes that may occur in the fetus and may result in miscarriage, fetal malformation, fetal death, neonatal death, infant death, permanent major newborn damage, permanent major autoimmune damage, permanent cognitive damage, permanent impairment of the immune health, and unleashing of infections and cancers.”
Just how concerning is the VAERS data so far? Dr. Thorp created a chart to compare the rate of miscarriages and fetal deaths (defined together as “pregnancy loss”) per month reported to the system for the COVID shots as compared to all other shots.
As you can see, we have seen 50 times the rate of reporting per month of miscarriages for this vaccine than the other vaccines put together. Thorp mentioned on my show that lest people think he opposes vaccines, he particularly recommends the flu and pertussis vaccines to his pregnant patients. You can see the rate of reporting for pregnancy loss among those shots is very low.
Now look at the rate of fetal malformations that have been reported to VAERS for COVID vaccines as compared to others.
Thorp requested that anyone who had the jab pushed on her in her pregnancy and believes she has suffered adverse effects in herself, her pregnancy, or her newborn to please contact him at jathorp@bellsouth.net.
Given that Scotland seemed to have experienced the most obvious safety alarm signal, why aren’t they looking into any of this? Well, in the richest of ironies, Glasgow Royal Fertility Clinic, one of the top fertility clinics in Scotland, has announced it will not serve any women without the shot. Why do they so badly not want a control group from which to study?
Those who believe in the freedom of bodily autonomy are celebrating a slew of recent court rulings enjoining the Biden administration’s injection mandate. However, no GOP state attorney general has bothered to fight the equally immoral, illogical, and inhumane mask mandates that are still in place. Despite nearly two years of evidence that strict mask-wearing has zero effectiveness in stopping the spread, the mandates on 2-year-olds on planes and in many schools still continue. Slovakia is a perfect case study of the mask mendacity.
On May 13, 2020, the Atlantic published an article lauding Slovakia for, at the time, having the lowest per-capita COVID death rate in Europe. The article’s prediction should now be the laughingstock of the world:
When this pandemic ends, and when the reckoning over how the world responded invariably begins, Slovakia will likely be among those highlighted as a success story, whereas the United States—which was supposed to be the country best prepared for such a crisis—will be remembered as among those that suffered the worst. How Slovakia was able to flatten its curve comes down to more than just quick decision making and the widespread adoption of face masks. Perhaps the greatest lesson to be learned from Slovakia is of the value of leading from the front.
Well, that was before Slovakia’s first winter wave. One can excuse people for mistaking low spread at the time for mask efficacy rather than the fact that the country just didn’t get its turn yet. But for countries to continue this inhumane mandate despite what we now know demonstrates that masks are not a means to public health but an end in themselves of tyranny.
At over 2,000 new cases per million per day, according to Our World in Data, Slovakia now has more cases per capita than any country in the world. To put this in perspective, that is almost three times the level of the winter peak in the U.S., a country that has not exactly performed well in the pandemic!
It’s true that some individual states closer to the size of Slovakia have had more severe waves. However, even the worst counties in the upper Midwest are tracking about 1,200 new cases per million per day.
And here is the epidemiological curve presented by the inimitable Ian Miller, juxtaposed to policy solutions:
It’s not just Slovakia. Wherever you turn in Europe, both masks and vaccine mandates have failed miserably, and the spread is now worse than ever. Belgium is now six weeks into the new mask mandate, and it has more cases than ever before, even though the Belgians already suffered one of the deadliest waves in all of Europe. Oh, and 87.4% of adults are vaccinated.
To begin with, the CDC, as late as May 2020, was citing the 10 randomized controlled trials that showed “no significant reduction in influenza transmission with the use of face masks.” The Centre for Evidence-Based Medicine at Oxford also summarized six international studies that “showed that masks alone have no significant effect in interrupting the spread of ILI or influenza in the general population, nor in healthcare workers.”
The only randomized controlled trial studying mask efficacy against COVID published last year was the now famous Danish study that failed to show any meaningful reduction in spread from mask-wearing. Then, several months ago, the media trumpeted a large study done in Bangladesh that seemed to show efficacy. Well, now that the authors have released the actual data, we see that indeed no such claim can be made from the study. It turns out that out of over 340,000 individuals over a span of eight weeks, there were only 20 fewer cases of COVID detected in the mask group over the control group – 1,106 symptomatic individuals confirmed seropositive in the control group and 1,086 such individuals in the treatment group.
Even these results are hard to interpret because of numerous confounding factors. University of California Berkeley professor Ben Recht critiqued the study as follows:
This study was not blinded, as it’s impossible to blind a study on masks. The intervention was highly complex and included a mask promotion campaign and education about other mitigation measures including social distancing. Moreover, individuals were only added to the study if they consented to allow the researchers to visit and survey their households. There was a large differential between the control and treatment groups here, with 95% consenting in the treatment group but only 92% consenting in control. This differential alone could wash away the difference in observed cases. Finally, symptomatic seropositivity is a crude measure of covid as the individuals could have been infected before the trial began.
Given the numerous caveats and confounders, the study still only found a tiny effect size. My takeaway is that a complex intervention including an educational program, free masks, encouraged mask wearing, and surveillance in a poor country with low population immunity and no vaccination showed at best modest reduction in infection.
It’s not OK for Republican-controlled states to continue to ignore the facts that masks are inhumane and they simply don’t work. Consider the fact that Head Start has now mandated masks on 2-year-olds, many of whom have special needs. Oregon has moved to make its mask mandate permanent. Why are no red state governments at least suing against the federal mandates, and why are so few red states even banning mask mandates within the states?
The courts are all political. They only responded to the lawsuits against the vaccine mandate when they saw robust political opposition within the political branches of the red states. They see no such opposition regarding the mask mandates. Thus, absent a unified effort from state attorneys general, they are unlikely to respond to a handful of individual lawsuits. The same legal rationale denying the feds the power to force vaccines also denies them the power to cover our breathing holes. But the courts only respond to political momentum.If nearly two years of masking failing to work anywhere is still not enough to end the most invasive human mandate of all time, then we truly are no longer a free people.
A tale of two drugs. One has become the standard of care at an astronomical cost despite studies showing negative efficacy, despite causing severe renal failure and liver damage, and despite zero use outpatient. The other has been safely administered to billions for river blindness and now hundreds of millions for COVID throughout the world and has turned around people at death’s doorstep for pennies on the dollar. Yet the former – remdesivir – is the standard of care forced upon every patient, while the latter – ivermectin – is scorned and banned in the hospitals and de facto banned in most outpatient settings. But according to the NIH, a doctor has the same right to use ivermectin as to use remdesivir. And it’s time people know the truth.
Although the NIH and the FDA didn’t officially approve ivermectin as standard of care for COVID, it is listed on NIH’s website right under remdesivir as “Antiviral Agents That Are Approved or Under Evaluation for the Treatment of COVID-19.” It is accorded the same status, the same sourcing for dosage recommendations, and the same monitoring advice as remdesivir … except according to NIH’s own guidance, remdesivir has a much greater potential for severe reactions in the very organs at stake in a bout with acute COVID.
Now, let’s take a closer look at the details.
As you can see, they admit that remdesivir causes renal and liver failure! One of the symptoms is “ALT and AST elevations,” which are indications of liver damage. Is that really the drug you want when someone is at risk for a cytokine storm and thrombosis? They even have a monitoring requirement for these side effects. Also, it does have some drug interactions as well.
Now, let’s move on to the ivermectin side effects.
Notice how the NIH is essentially saying it has no side effects by the fact that it prefaces the section by noting the drug is “generally well tolerated,” a distinction not accorded to remdesivir. Then it proceeds to list the same boilerplate GI and nausea warnings on every drug under the sun. There are almost no drug interactions and ZERO specific guidance for monitoring!
Just looking at the NIH’s own table, why in the world would remdesivir be the expensive mandatory standard of care and ivermectin, buttressed by 64 studies, be relegated to hemlock status even for patients about to die and with no other options?
Yes, we get the message – every one of those studies is supposedly low-powered, a fraud, and all the thousands of doctors turning people around on ivermectin are some how frauds even though they have nothing to gain and everything to lose from pushing it. But if that is our standard for ivermectin, it raises the obvious question about remdesivir. How could remdesivir not only be approved but made the standard of care when it has negative efficacy in trials, has a negative recommendation from the WHO, and, by the NIH’s own admission, causes liver and kidney failure?
Even if the medical establishment dismisses the preponderance of evidence and reality of the past 18 months, with ivermectin saving so many people, just from a safety standpoint, why would they not allow people to at least try something this safe while forcing on them a dangerous drug like remdesivir? In addition, these are the same hospitals that administer Olumiant, which has a rare FDA black box warning for blood clots, even though these very patients are at high risk for a pulmonary embolism and other clotting disorders?
In other words, there is no way anyone can justify the war on ivermectin (and every other cheap treatment that has been and will be proposed) as being rooted in anything related to medicine and science. If that were the case, the medical establishment would be dead set against remdesivir and Olumiant. Moreover, to the extent remdesivir has any efficacy that is worth its risk, it would be outpatient during the viral stage. There is quite literally no scientific way remdesivir can work in the pulmonary inflammation stage. Unlike ivermectin, which tones down inflammatory cytokines such as IL-1beta and IL-10 as well as tumor necrosis factor alpha, remdesivir has no anti-inflammatory qualities.
Gee, is there any wonder hospitals will fight patients in court – including those whom they already recommend to remove from life support – to not even try ivermectin as a last resort?! So much for the desire to flatten the curve of hospitalizations. They want people in the hospital! If they really cared about the run on hospitals, they’d promote treatments that work early and outpatient so that nobody would need to come to the hospital.
Here’s one other strong piece of evidence that this is not about any shortcoming of ivermectin, but stems from unrelenting war on anything off patent that might work, in order to run interference for expensive, dangerous, and ineffective tools of big pharma. Let’s go back to that NIH chart of potential antiviral drugs for COVID. There is actually a third one on that list aside from remdesivir and ivermectin.
Nitazoxanide, much like ivermectin, is a (potentially) cheap off-patent anti-parasitic that has been praised for years as a very safe, broad-spectrum anti-parasitic mechanism and is written about glowingly in studies. And it actually has an even longer and more direct precedent of research and clinical use against viruses than even ivermectin. It is the standard of care for norovirus and rotavirus in Brazil and has shown promise against not just flus and hepatitis, but coronavirus colds, SARS, and MERS. This research has been known even in the media for well over a year! Gee, we have an antiviral that is so safe it’s given to young kids for viral diarrhea and has been known to work against coronaviruses. Yet our government has refused to pursue any meaningful research for 18 months!
Originally, it was as cheap as ivermectin, but one company seems to have bought it up, and now it is prohibitively expensive in the U.S. However, were the government to promote it, this off-patent drug could easily be mass-produced for pennies on the dollar and costs just a few dollars for a full regimen in Mexico and Brazil.https://playlist.megaphone.fm/?e=BMDC5574376707
Notice that, just like with ivermectin, the NIH prefaces the side effects section on nitazoxanide by saying it is “generally well tolerated” and then proceeds to list the boilerplate of typical minor side effects that are disclosed for every drug under the sun. Anyone merely looking at this NIH page alone can see how the government and medical establishment’s treatment of remdesivir vs. every other therapeutic that has been tried is built upon control, greed, and something much darker than that. Now, just remember, these are the same people who will look you in the eye and say the shots are 100% effective and carry zero risk. It’s all in the $cience. What is self-evident from the NIH’s disclosure, which was updated as late as July 2021, is that ivermectin and nitazoxanide work for a lot more than just parasites. It’s primarily the political parasites that fear that those drugs.
“Basically, our organization is run on COVID money now.” ~ Chris Croce, senior associate scientist, Pfizer (Project Veritas undercover video)
We were lied to … big-time.
Back in December, the CDC stated clearly that the Pfizer-BioNTech COVID-19 vaccine “was 95.0% effective (95% confidence interval = 90.3%–97.6%) in preventing symptomatic laboratory-confirmed COVID-19 in persons without evidence of previous SARS-CoV-2 infection.” Indeed, in late March, Director Rochelle Walensky promised, “Our data from the CDC suggest that vaccinated people do not carry the virus.” Even those who had questions about transmission among the vaccinated were only concerned about asymptomatic transmission, whereas now we see that the vaccinated can contract the infection symptomatically.
Fast-forward three-quarters of a year through the era of mass vaccination, and a Harvard researcher could not find any correlation between vaccination rates and COVID case rates after examining 68 countries and 2,947 counties in the United States. “At the country-level, there appears to be no discernible relationship between percentage of population fully vaccinated and new COVID-19 cases in the last 7 days,” concluded the authors in the study published in the European Journal of Epidemiology. “In fact, the trend line suggests a marginally positive association such that countries with higher percentage of population fully vaccinated have higher COVID-19 cases per 1 million people.”
The authors continue:
Notably, Israel with over 60% of their population fully vaccinated had the highest COVID-19 cases per 1 million people in the last 7 days. The lack of a meaningful association between percentage population fully vaccinated and new COVID-19 cases is further exemplified, for instance, by comparison of Iceland and Portugal. Both countries have over 75% of their population fully vaccinated and have more COVID-19 cases per 1 million people than countries such as Vietnam and South Africa that have around 10% of their population fully vaccinated.
Of the top 5 counties that have the highest percentage of population fully vaccinated (99.9–84.3%), the US Centers for Disease Control and Prevention (CDC) identifies 4 of them as “High” Transmission counties. Chattahoochee (Georgia), McKinley (New Mexico), and Arecibo (Puerto Rico) counties have above 90% of their population fully vaccinated with all three being classified as “High” transmission. Conversely, of the 57 counties that have been classified as “low” transmission counties by the CDC, 26.3% (15) have percentage of population fully vaccinated below 20%.
It’s also important to keep in mind that when calculating the data, the authors used a sensitivity analysis by applying a one-month lag on the percentage population fully vaccinated so that people wouldn’t be considered fully vaccinated until 14 days after the second dose. However, studies have shown that this is the most vulnerable time for getting the virus. Why should that be blamed on the lack of vaccination rather than on the vaccine? So if anything, the numbers are likely even more unfavorable to the vaccine than this analysis suggests.
“The sole reliance on vaccination as a primary strategy to mitigate COVID-19 and its adverse consequences needs to be re-examined, especially considering the Delta (B.1.617.2) variant and the likelihood of future variants,” conclude the authors, including the lead researcher from Harvard’s Center for Population and Development Studies and a student researcher from Canada. The study did not factor in which vaccine predominated in a given country, but rather looked at the top-line vaccination rates, which include several vaccines that likely vary in terms of effectiveness.
How can these mandates hold up in court given that they likely don’t even pass the rational basis test of fulfilling a state’s vital interest of stopping the spread of a virus?
A July study of Israel perfectly embodies the complete lack of efficacy from this vaccine, especially in recent months. In a study published in a European CDC journal, Israeli researchers in one hospital found studies a serious outbreak among a group of patients and staff of whom 96% were vaccinated. 42 patients and staff wound up getting COVID from a vaccinated dialysis patient who had an extremely high viral load. According to the authors, “Of the 42 cases diagnosed in this outbreak, 38 were fully vaccinated with two doses of the Comirnaty vaccine, one was recovered with one vaccination and three were unvaccinated.” All patients and family members wore surgical masks and all staff wore N-95s with face shields and gloves.
Overall, “Among the patients (median age: 77 years; range: 42–93; median time from second vaccine dose to infection: 176 days; range: 143-188), eight became severely ill, six critically ill and five of the critically ill died.” All of the unvaccinated cases were described as mild, even though one of them was in his 80s. The Israelis are using this to push for boosters, but what it really demonstrates is that the vaccine has been a dud, especially for those who needed it the most.
The reality is that the notion that protection against serious illness is holding up, even as the vaccinated spread the virus more than ever, is collapsing by the day. According to the Associated Press, hospitalizations are surging in New England. The five states with the highest percentage of a fully vaccinated population are all in New England. At some point, it becomes hard to blame a worse spread than pre-vaccination on the few remaining unvaccinated adults without first investigating whether the vaccine itself made the virus worse.
For those of you who couldn’t believe that the government’s war on ivermectin and every other treatment was rooted in a sinister motivation, its new attack on the monoclonal antibodies should indelibly cement the terrifying thought in your mind. The government and the media are now using the same attack pattern on the monoclonal antibody treatment that they used on hydroxychloroquine and ivermectin now that it has become popular with people desperate for treatment – vaccinated and unvaccinated alike.
On Sept. 14, the Biden administration announced that the feds would be cutting the number of monoclonal treatments per week in the southern states and reallocating them as part of a broader plan to start rationing the treatments. For example, in Florida, HHS issued an allocation for the week of Sept. 13 of 3,100 doses of BAM/ETE treatments and 27,850 doses of REGN-COV. As Florida Gov. Ron DeSantis said in a press conference last week, this would effectively reduce Florida’s allocation by 50%. The federal agency did this without any warning or indication that there was a shortage.
Then, last Thursday, White House press secretary Jen Psaki explained the move as follows: “Our supply is not unlimited and we believe it should be equitable.” HHS then followed up with an explanation of the policy of “equity.”
But wouldn’t you focus on where it’s needed at a given time rather than blind “equity”? Also, Biden promised just days earlier during the announcement of his vaccine mandate to boost monoclonal distribution by 50%.
Well, here is the answer to the enigma: In that same announcement, Biden warned, “If these governors won’t help us beat the pandemic, I’ll use my power as president to get them out of the way.” Is the federal takeover of the monoclonals his ace in the hole? And why wouldn’t the government just produce more? We have spent trillions of dollars on welfare, shutdowns, and vaccines that failed so miserably that people who already got the shots still need the monoclonals! So why not put the funding into the monoclonals?
Well, if you are trying to ascertain the motivation of government always watch carefully for its stenographers in the media to follow up with the psy-ops on the general public, which will reveal the true messaging. Once you read this New York Times article, you will see clearly that this is really not about “equity” or some concern over supply. In an article titled, “They shunned COVID vaccines but embraced antibody treatments,” the NYT essentially frames the monoclonals as some right-wing solution that is only for those who didn’t want to get the vaccine.
Some Republican governors have set up antibody clinics while opposing vaccine mandates, frustrating even some of the drugs’ strongest proponents. Raising vaccination rates, scientists said, would obviate the need for many of the costly antibody treatments in the first place. The infusions take about an hour and a half, including monitoring afterward, and require constant attention from nurses whom hard-hit states often cannot spare.”It’s clogging up resources, it’s hard to give, and a vaccine is $20 and could prevent almost all of that,” said Dr. Christian Ramers, an infectious disease specialist and the chief of population health at Family Health Centers of San Diego, a community-based provider. Pushing antibodies while playing down vaccines, he said, was “like investing in car insurance without investing in brakes.”
Except it’s simply not true. The vaccines are no longer working, especially for those who got them early on — particularly the elderly — and many of the people who got them badly need treatment. As Gov. DeSantis reported, the majority of those seeking monoclonals are vaccinated, a fact I have verified in the facility closest to me in Baltimore. Here are the statistics the Florida government publicized at last week’s press conference:
At our Broward site, 52% of the patients that have received treatment have been vaccinated, 69% of those over 60 that have received treatment at the Broward site had been vaccinated. In Miami Dade almost 60% of everybody that’s been treated at the Tropical Park site has been vaccinated. And 73% of the patients treated at the state site in Tropical Park that are over the age of 60 have been vaccinated.
So again, it’s the exact opposite of what the media and the Biden administration are saying. The vaccines cost a fortune and failed. Now these same people need treatment. The same government officials rationing the monoclonals have already scared 99% of doctors away from prescribing and pharmacists from filling cheap off-patent drugs that have cured the few people who can access them. The monoclonals are made by the cool kids at big pharma and are approved by the government. Except our government paid them off up front and then refused to even make the public aware of their existence. Thus, even things produced by big pharma are now attacked, so long as they actually work and people begin successfully using them.
It’s so cute to watch the government and media suddenly become concerned about expensive treatments after spending billions on the vaccines. There is a simple solution, and that would be mass production of ivermectin and encouraging all physicians to treat everyone early with it and other cheap drugs. But now that the government has essentially banned them, the monoclonals are the only show in town. This is where the Biden administration wants to place Americans they don’t like into a death trap.
Texas Montgomery County Judge Mark Keough warned that this is not about a lack of supply. “The manufacturer has confirmed supplies are ample but due to the Defense Production Act, the White House and its agencies are the only entities who can purchase and distribute this treatment,” wrote Keough on Facebook.
With the war on any and all forms of early treatment, ask yourself this question: Does our government really want the pandemic to end?
Why should the estimated one-third of Americans who have already contracted the virus still be treated like ticking time bombs? How much longer will the government get away with denying the science behind immunity from infection?
The isolation of all human beings as a strategy to deal with this virus began with the novel assumption of mass asymptomatic spread, a hypothesis now disproven by studies on transmission. Now, the mandatory masking and isolation are continuing without question based on a shocking lie that the one-third of the country who have already gotten the virus – despite the masks and lockdowns, by the way – are not immune to the virus.
As more and more studies have come out showing that prior infection confers long-lasting immunity – not just the 90 days we are told by the government – the purveyors of panic and tyranny have sought to use the focus on several supposedly new variants to deny the presumed immunity from prior infection. However, a new comprehensive study from Harvard Medical School and Boston University researchers should put this latest myth to rest.
The researchers took blood samples from people who had the virus from March 3 to April 1, 2020, long before the new variants were discovered, which allowed them to presume they all had the original Wuhan strain. They found the S-specific memory B cells “conferring robustness against emerging SARS-CoV2 variants” – the U.K. (B117) & South African (B1351) variants.
“Loss of protection against overt or severe disease is not an inevitable consequence of a waning serum antibody titer,” wrote the authors. “This atlas of B cell memory therefore maps systematically a crucial component of the long-term immune response to SARS-CoV-2 infection.”
In other words, the inherent immune system full of B cells (in addition to T cells) provides robust immunity not just long after the antibody titers wane from the original infection, but also against emerging strains of the virus.
There has been much discussion over whether the vaccine confers immunity against the new variants, but the more important fact is that previous infection confers such immunity, as is the case with nearly every virus. Indeed, cases have plummeted in South Africa and England precisely since the new variants have been discovered, which would be difficult without natural immunity from the prior waves working against the new variants.
In Denmark, the U.K. variant composes roughly three-quarters of all cases, yet the country is averaging one death per day over the past 7 days. The same holds true for a number of states in America.
A retrospective observational study of 14,840 COVID-19 survivors in Austria found just a 0.27% reinfection rate during the second wave. “Protection against SARS-CoV-2 after natural infection is comparable to the highest available estimates on vaccine efficacies,” concludes the study, published in the European Journal of Clinical Investigation.
It’s also important to remember that, as with other viruses, immunity doesn’t necessarily mean you can’t test positive again, but that you won’t experience serious symptoms even if you do. The goal is not to prevent colds and flus, but to pre-empt serious illness and death. “With follow‐up on mortality available until December 23, only one 72‐year‐old woman died two days after her tentative re‐infection diagnosis,” observed the authors of the Austrian study. “She was not hospitalized and according to her medical records her cause of death (‘acute vascular occlusion of an extremity with rhabdomyolysis’) was not causally attributed to COVID‐19.”
As the Los Angeles Times reported already in February, with an estimated 35% of Americans already infected (up to 50% in Los Angeles!), “the biggest factor” driving the plummeting of cases “paradoxically, is something the nation spent the last year trying to prevent.” That is herd immunity. As illogical as it was to lock down all Americans last year, regardless of whether they were sick, it’s downright insane to continue masking people who already had the virus AND have no current symptoms.
We’ve already learned from reams of medical research that asymptomatic individuals rarely drive outbreaks. Coupled with already having been infected, the likelihood of a recovered COVID patient both getting the virus and transmitting it is so low that it makes further masking of these people unconscionable.
With this thought fresh in your mind, now consider the insane abuse our government continues to foist upon kids by masking them seven hours a day in school. You can have a child who already had the virus and currently has no symptoms, yet he is still forced to wear a mask. What’s worse, with mass testing of children, yet extremely low rates of infection in recent weeks, the chance of false positives is extremely high. Last week, Professor Jon Deeks, a biostatistician from the University of Birmingham, told the U.K. Telegraph, “It seems likely that over 70% of positive test results are false positives, potentially many more.”
So, children continue to be masked or even removed from school with no symptoms, based on faulty testing, predicated on a false assumption of mass asymptomatic spread – when so many of them already have immunity. In other words, this cycle can go on forever.
Just how big a lie is mass asymptomatic spread? Last month, the Federalist’s Georgi Boorman trenchantly observed how the CDC mistakenly admitted that its entire premise of masking and isolating asymptomatic people is based on a lie. While finally acknowledging in its Jan. 29 report the fact of insignificant levels of spread in schools, the CDC let the following genie out of the bottle:
“Children might be more likely to be asymptomatic carriers of COVID-19 than are adults. … This apparent lack of transmission [in schools] is consistent with recent research (5), which found an asymptomatic attack rate of only 0.7% within households and a lower rate of transmission from children than from adults. However, this study was unable to rule out asymptomatic transmission within the school setting because surveillance testing was not conducted” (emphasis added).
So, when it comes to explaining why children rarely spread the virus, the CDC settled on the principle that children usually get infected asymptomatically, which means very little transmission! That would apply to adults who don’t have symptoms, too, but the CDC will never concede that point. In fact, the low rate of transmission in that study includes both asymptomatic and pre-symptomatic cases. Nevertheless, despite the CDC admitting that kids, especially young kids, are not vectors of spread, it updated its guidance to continue recommending that children as young as two, aka babies, wear masks at child care facilities except for when they are eating and sleeping!
Which raises the question: With so many people already having had the virus and feeling healthy, what is the legal justification for using the police power of quarantine against those people? There is none, and there never has been a legitimate constitutional authority, yet they’ve done it anyway. In other words, if we don’t end this tyranny now, it will never end, because quarantine and masking are no longer a means but an end.
What can states do when the federal government not only keeps its border open, but directly invites the cartels and smugglers to bring in potentially millions of new migrants, along with cartel members, gangsters, and previously deported criminals? That is a question we never thought we’d have to grapple with, but it is of vital importance for our national security and communities.
In January, I laid out the constitutional case for states to secure the border when the federal government is actively working against border security, one of the foundational purposes for the states to create a federal government in the first place. Now, one Texas lawmaker is introducing a bill that could serve as the impetus for states actually securing some degree of control over the border.
On Monday, Texas state Rep. Bryan Slaton filed HB 2862, which would fund the completion of the border wall in Texas with state funds. The bill requires the governor to request reimbursement from the federal government. Such an effort would bolster the existing Operation Lone Star, in which Gov. Greg Abbott has deployed the Texas Rangers to the border.
The reason this bill is so important is because the Biden administration halted the construction of the border fence even while portions of the wall were still being built. The fact that parts of the wall were built non-contiguously has allowed the cartels to easily go around the fencing. Worse, as I reported last week, the cartels now have the advantage of using the new access roads built during the construction. Thus, the half-completed fencing, in some ways, leaves us more vulnerable than before the construction.
Overall, the Trump administration constructed 453 miles of new fencing – 373 miles of replacement fencing for existing designs that were dilapidated or easy to breach and 80 miles where no fencing existed. However, most of that fencing was in Arizona or in the El Paso sector, which includes far west Texas and New Mexico. Just 18 miles were completed in the Rio Grande Valley sector and zero miles were completed in the Del Rio and Laredo sectors, but 165 miles in those three sectors were under construction when Biden terminated the project. Del Rio, in particular, is a hot spot at this point.
It’s also important to build in Arizona. As the Cochise County sheriff told me in an interview, the fact that the wall and its infrastructure were halted midway through made things worse than they were before. Builders completely ripped out the old fencing to build new fencing, but now, with construction halted, there is nothing there, and illegal immigrants and smugglers can cross over with cars and enjoy the newly built access roads. “They literally just walked away from it,” said Sheriff Dannels.
What’s worse is that in Cochise County, the infrastructure in the low water crossings was not completed, which means that when the heavy rains come in a few months, the foundations will be destroyed, making it much more expensive to rebuild. Meanwhile, time is of the essence, as Sheriff Dannels is now counting close to 3,000 runners detected on his cameras per month, up from just 400 a month a year ago. His sergeant, Tim Williams, who runs the camera system, tells me the department is only apprehending about 35% of them. Due to the rugged terrain and remote areas, those crossing in areas of the border like Cochise are mainly criminals and drug runners – not the sort of people you want disappearing into the interior.
Arizona would be wise to follow up with its own bill to complete at least the existing infrastructure of the border wall. Likewise, other red states can chip in by appropriating small amounts of money to pool together in an effort to help these two border states shoulder the national burden. They can also crowdsource from private funds.
Such a national effort to complete the border wall would publicly embarrass the Biden administration and force an inflection point in our body politic regarding the border situation as a whole. States will be forced to choose between anarchy and security. The red states have no choice but to act before hundreds of thousands more teem through our border.
Don McLaughlin, mayor of Uvalde, Texas, 60 miles into the interior from the Del Rio border with Mexico, explained on my podcast how ranchers in his county are now being confronted by desperate smugglers.
“The ranchers are getting confronted more and more, their fences are getting cut, and their land is being trashed by the migrants,” said the border mayor. “What’s concerning is that they are getting bolder and bolder about coming to your house and demanding you give them food, you give them transportation, and you give them money. It’s a powder keg that’s going to blow up. It’s not a matter of if, it’s a matter of when somebody is going to get shot – whether it be a local citizen, a local rancher, or one of these immigrants coming across the ranches, because they’re getting braver and braver. And some of them, to be honest, are very aggressive when they approach you. We’re seeing more aggressiveness now than we’ve ever seen before.”
The anarchy that spills over on our side of the border obviously bubbles up from the Mexican side. Even the Mexican government has become exasperated with Biden. As Reuters reports, Mexico President AMLO referred to Biden as the “migrant president,” and his government is concerned at how Biden’s policies have created a sophisticated market for organized crime up and down the smuggling routes of Mexico.
Perhaps the red states can even work with Mexico to build the wall and make Biden pay for it!
American Family Association
American Family Association (AFA), a non-profit 501(c)(3) organization, was founded in 1977 by Donald E. Wildmon, who was the pastor of First United Methodist Church in Southaven, Mississippi, at the time. Since 1977, AFA has been on the frontlines of Ame
NEWSMAX
News, Opinion, Interviews, Research and discussion
Opinion
American Family Association
American Family Association (AFA), a non-profit 501(c)(3) organization, was founded in 1977 by Donald E. Wildmon, who was the pastor of First United Methodist Church in Southaven, Mississippi, at the time. Since 1977, AFA has been on the frontlines of Ame
American Family Association
American Family Association (AFA), a non-profit 501(c)(3) organization, was founded in 1977 by Donald E. Wildmon, who was the pastor of First United Methodist Church in Southaven, Mississippi, at the time. Since 1977, AFA has been on the frontlines of Ame
You Version
Bible Translations, Devotional Tools and Plans, BLOG, free mobile application; notes and more
Political
American Family Association
American Family Association (AFA), a non-profit 501(c)(3) organization, was founded in 1977 by Donald E. Wildmon, who was the pastor of First United Methodist Church in Southaven, Mississippi, at the time. Since 1977, AFA has been on the frontlines of Ame
NEWSMAX
News, Opinion, Interviews, Research and discussion
Spiritual
American Family Association
American Family Association (AFA), a non-profit 501(c)(3) organization, was founded in 1977 by Donald E. Wildmon, who was the pastor of First United Methodist Church in Southaven, Mississippi, at the time. Since 1977, AFA has been on the frontlines of Ame
Bible Gateway
The Bible Gateway is a tool for reading and researching scripture online — all in the language or translation of your choice! It provides advanced searching capabilities, which allow readers to find and compare particular passages in scripture based on





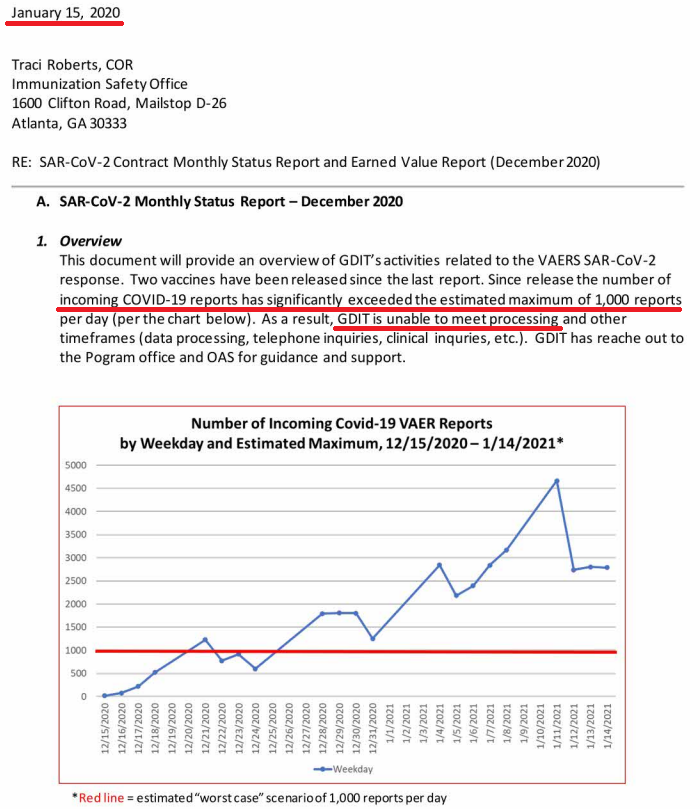


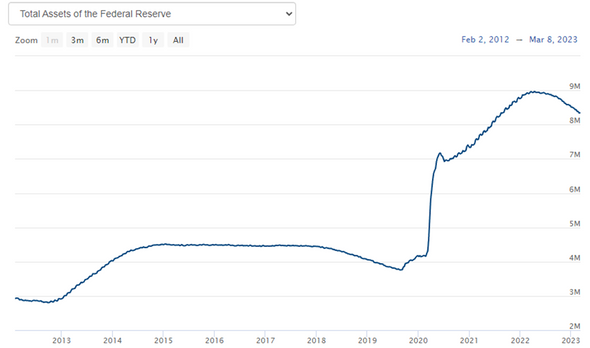



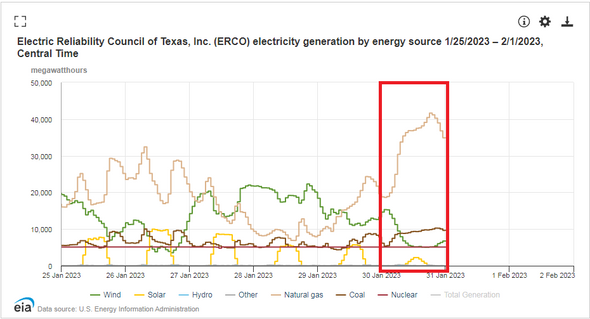

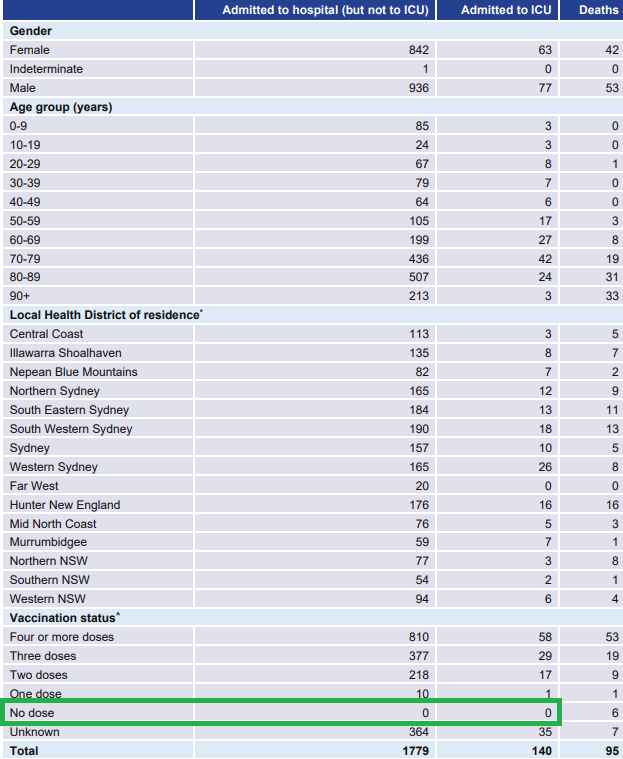
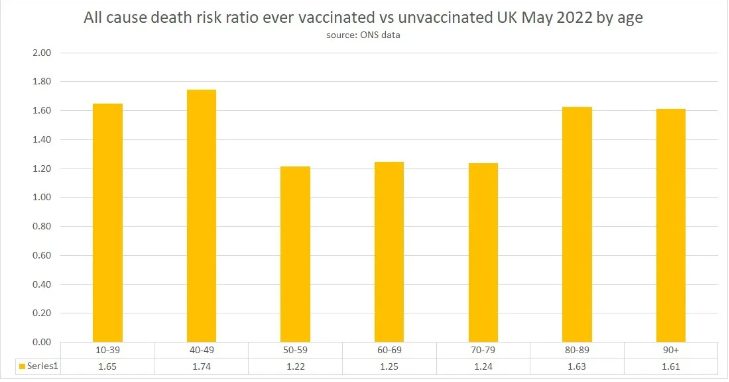

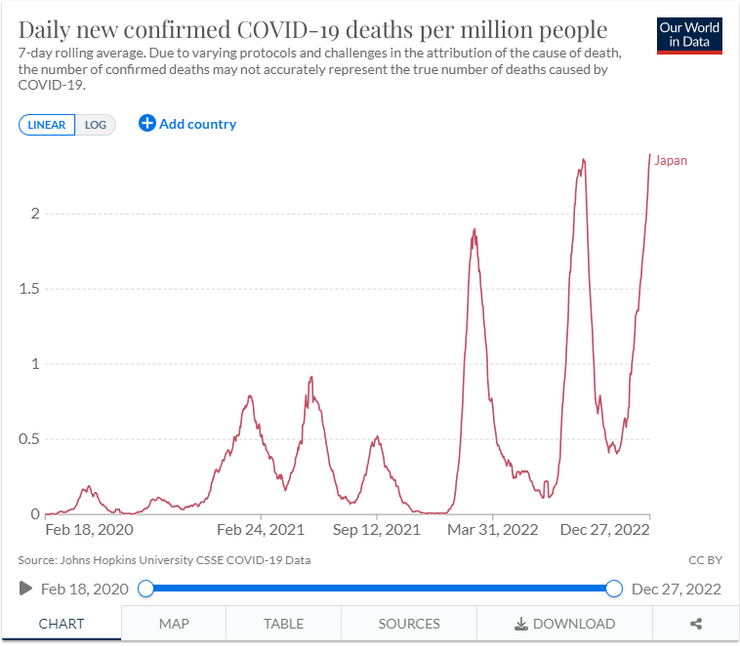
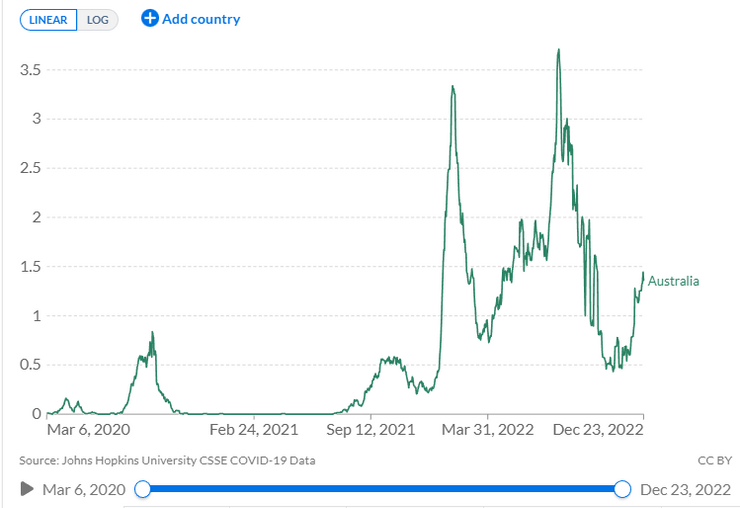
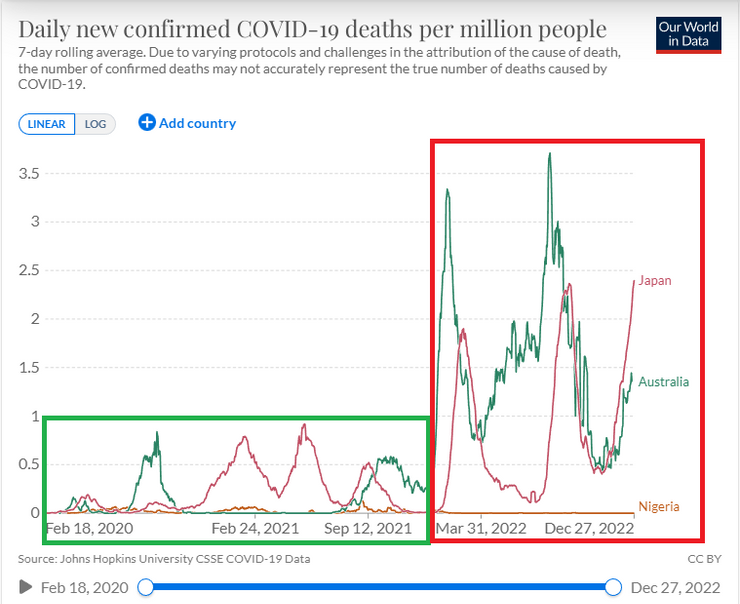
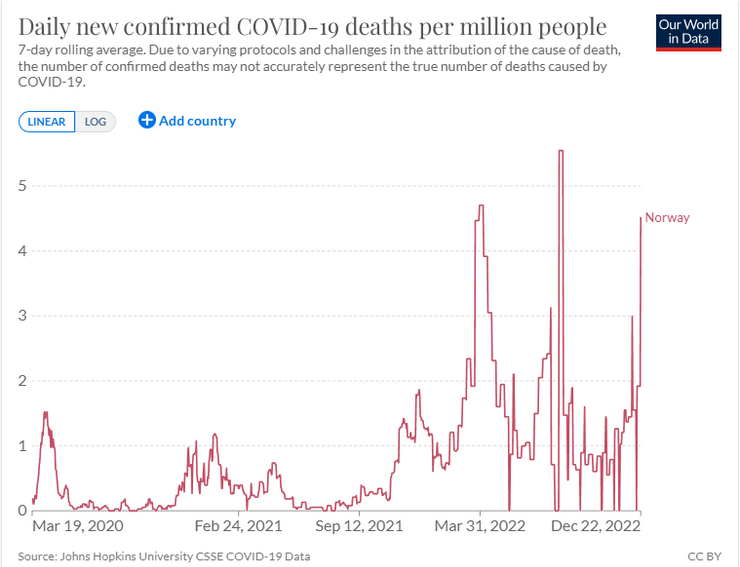
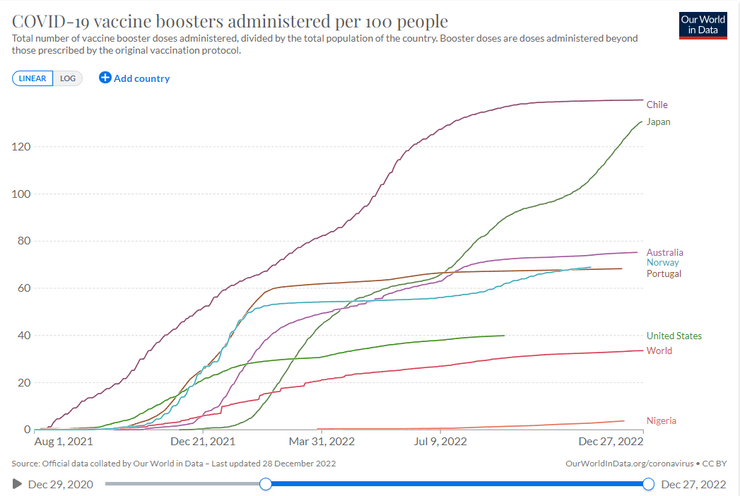



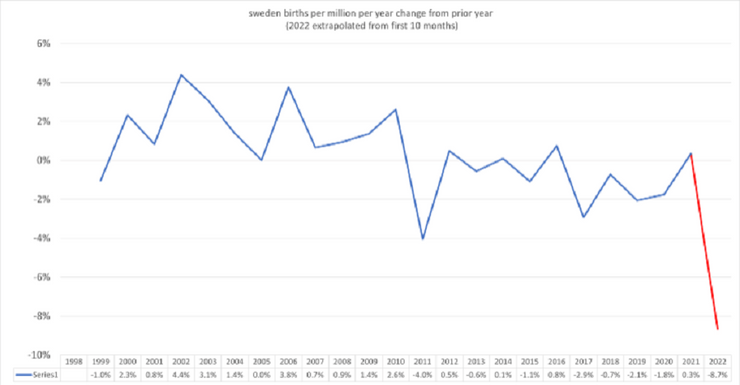
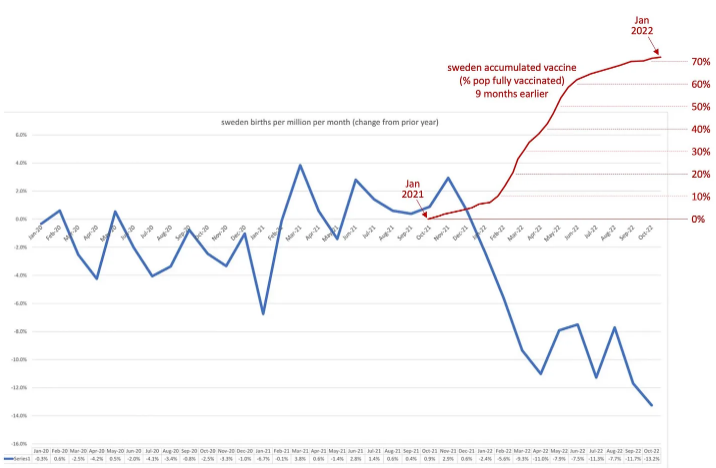
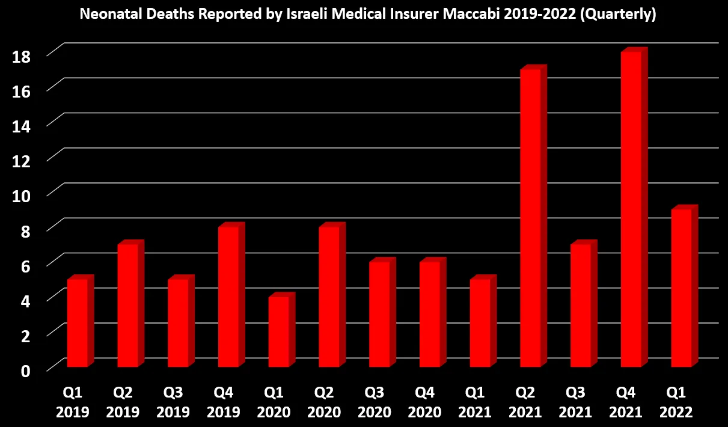


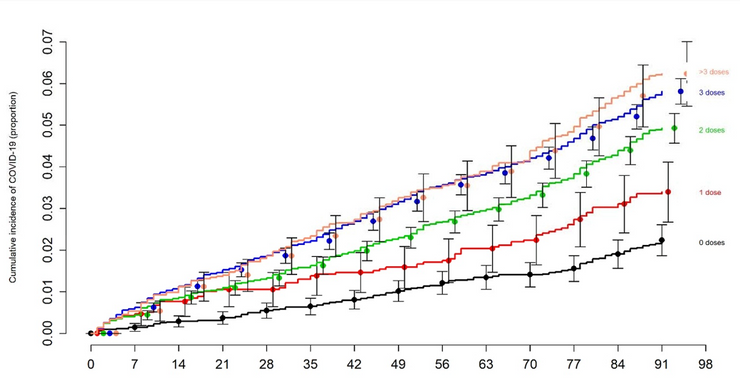
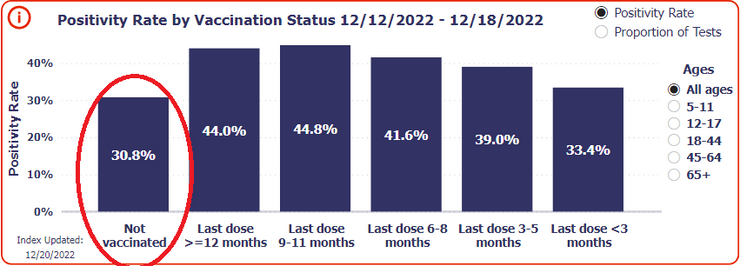
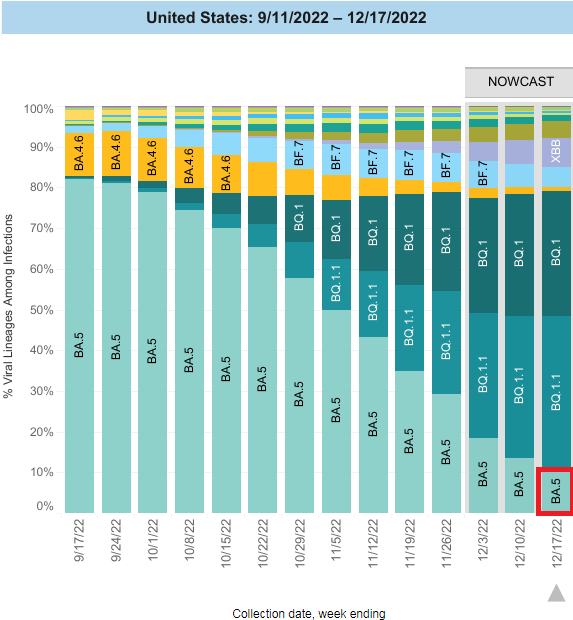



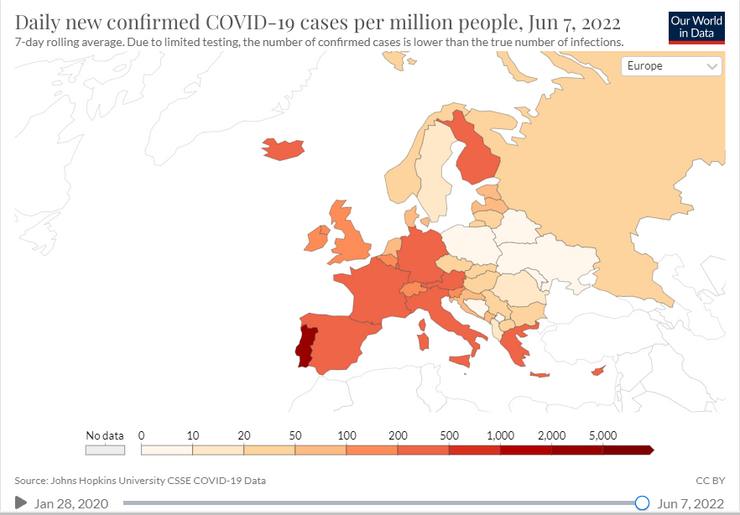
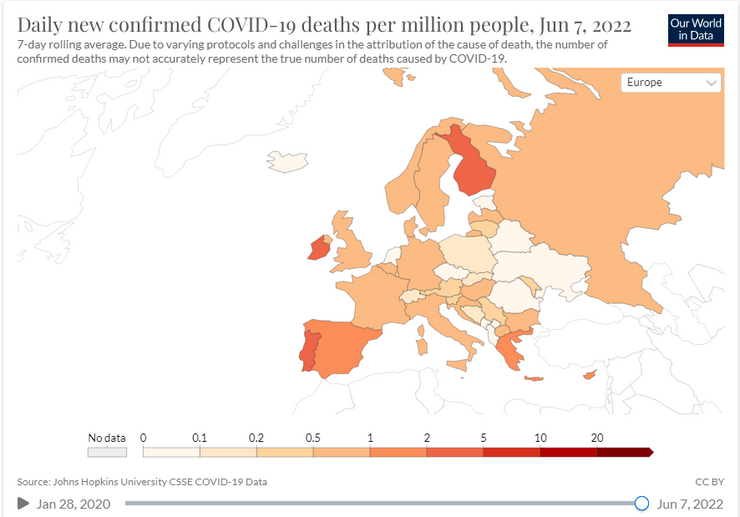
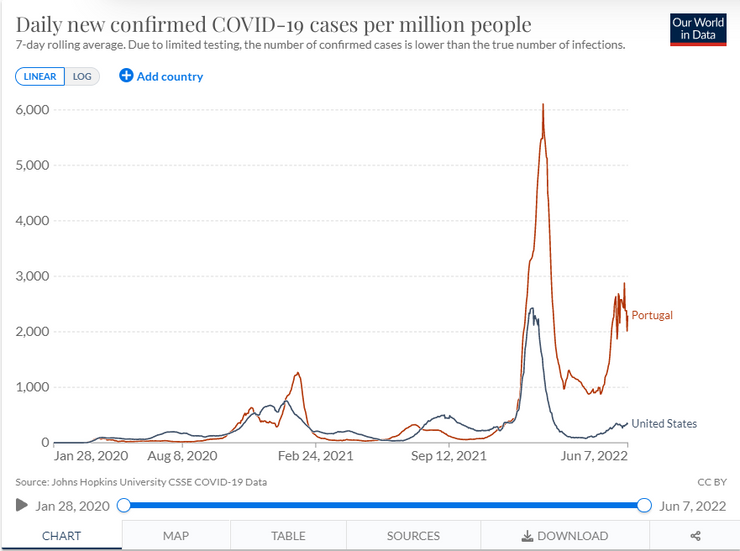
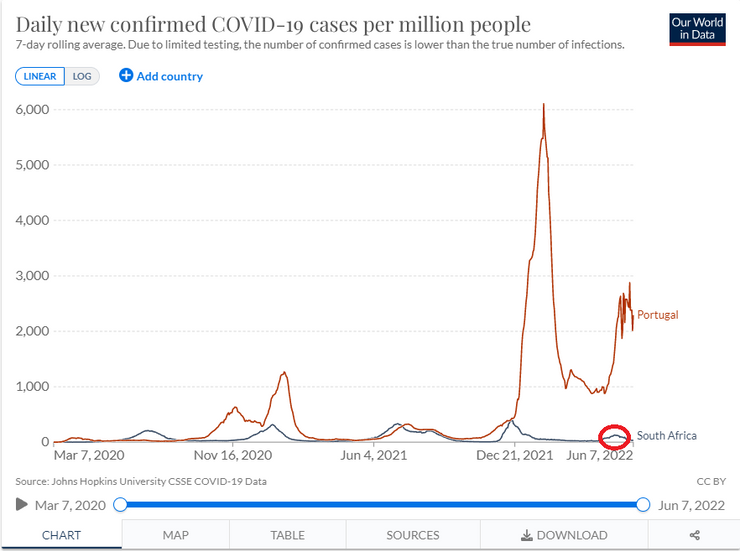
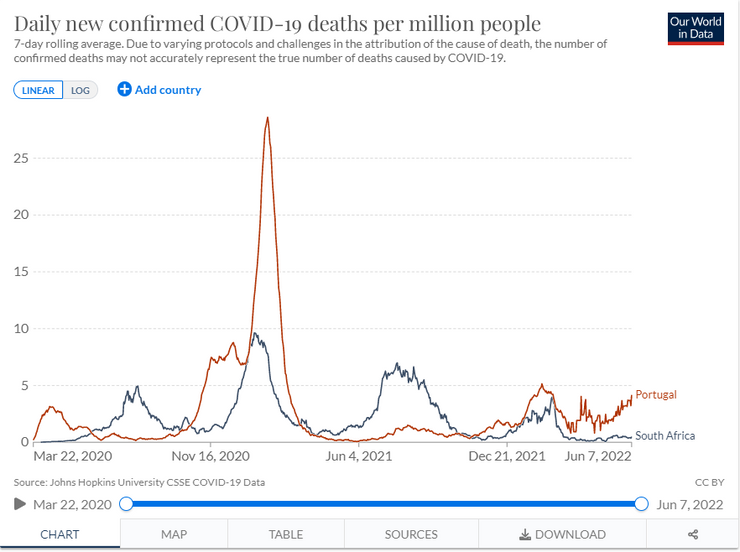
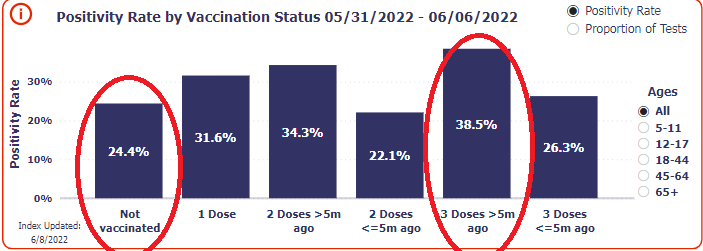
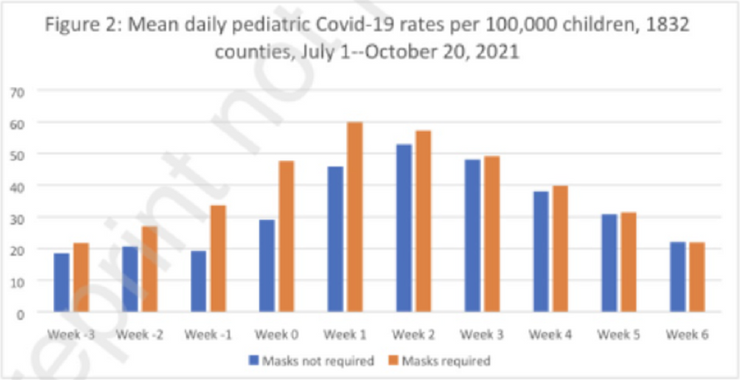



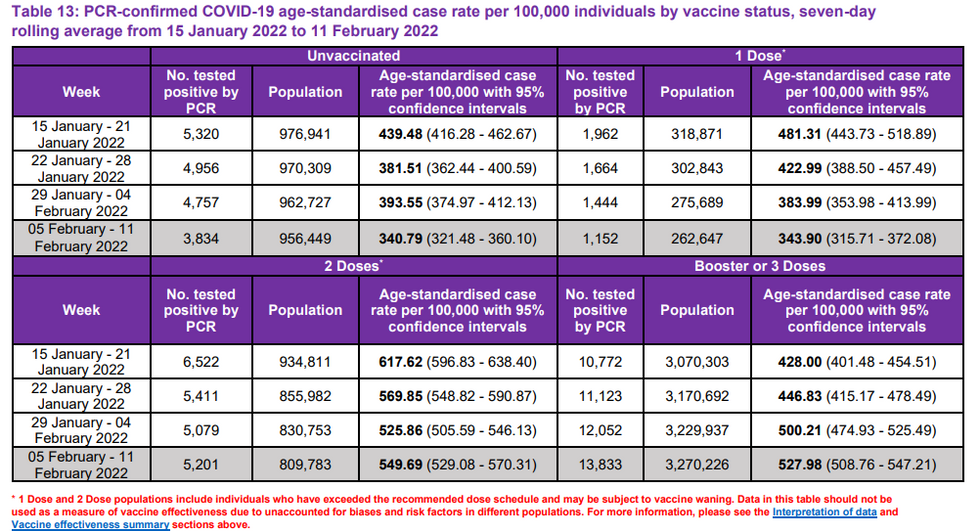
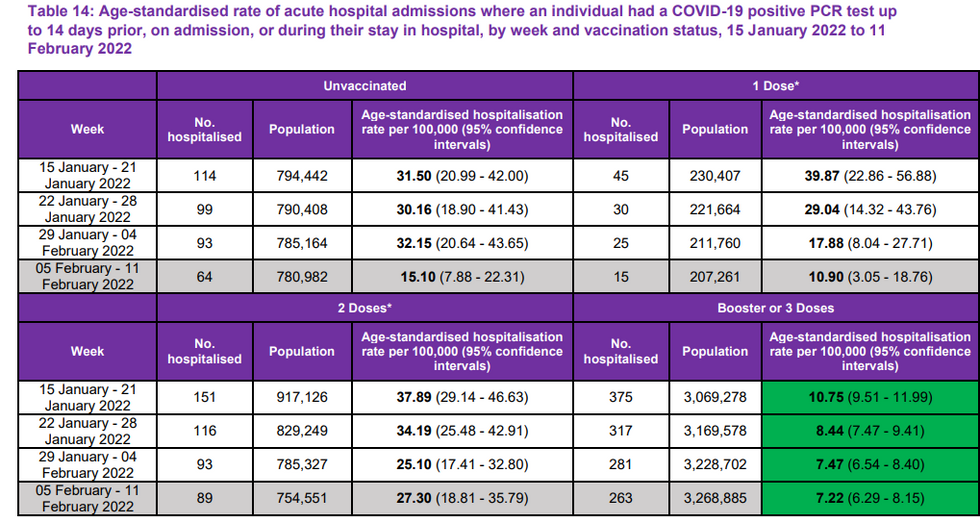
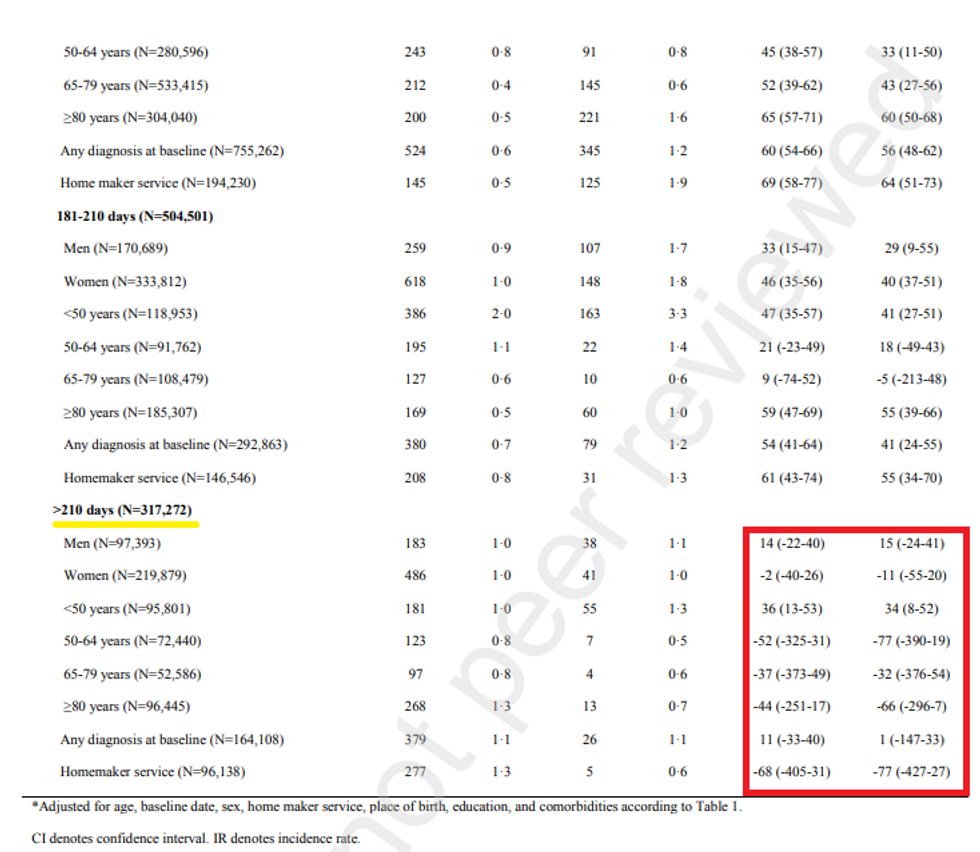
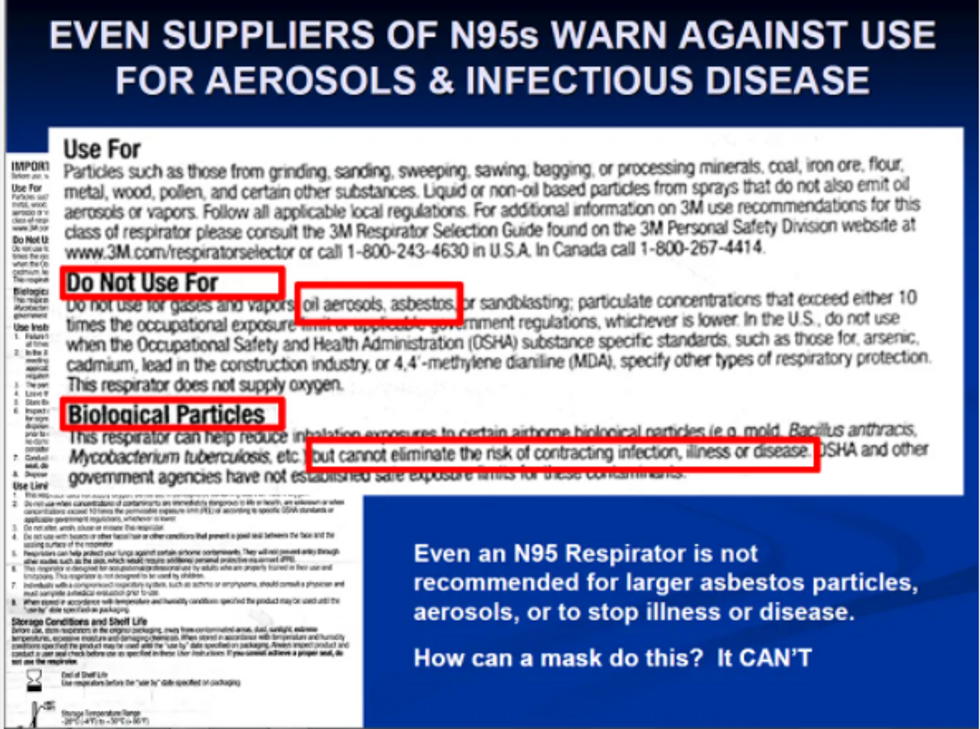
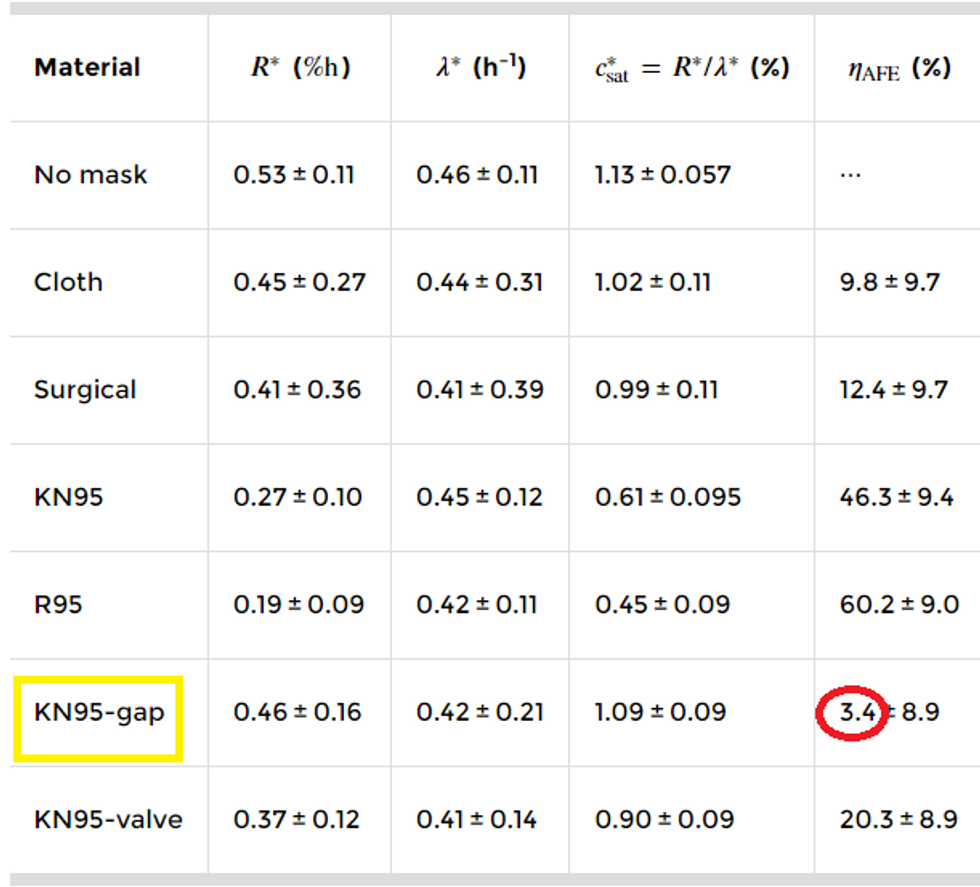

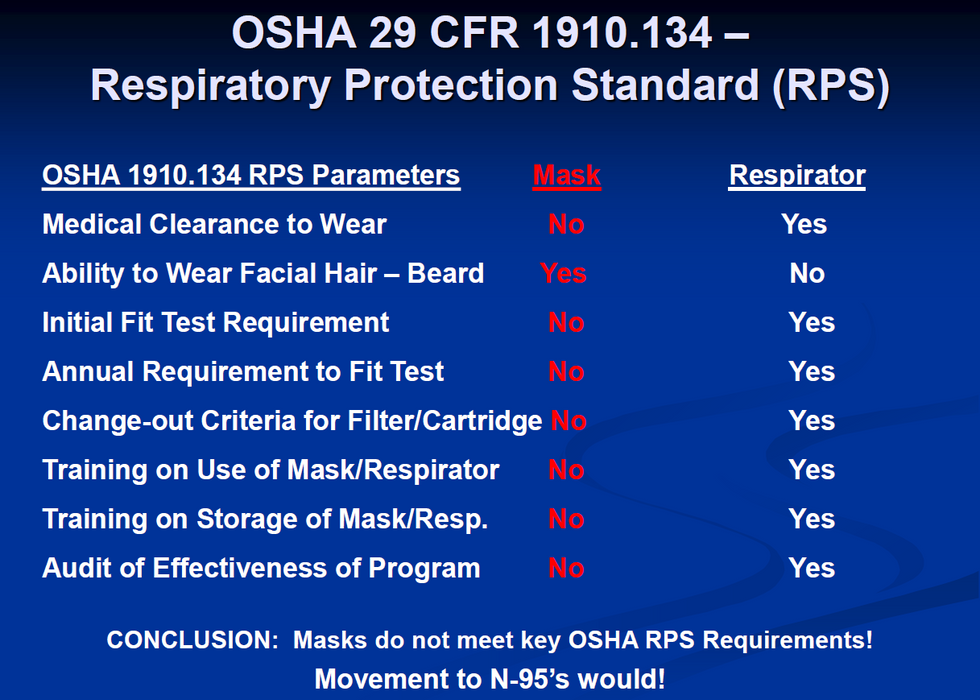
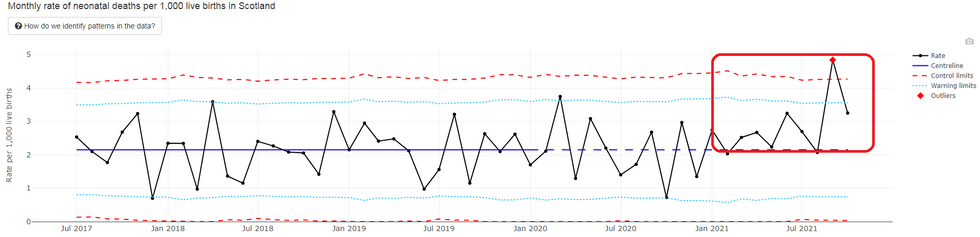

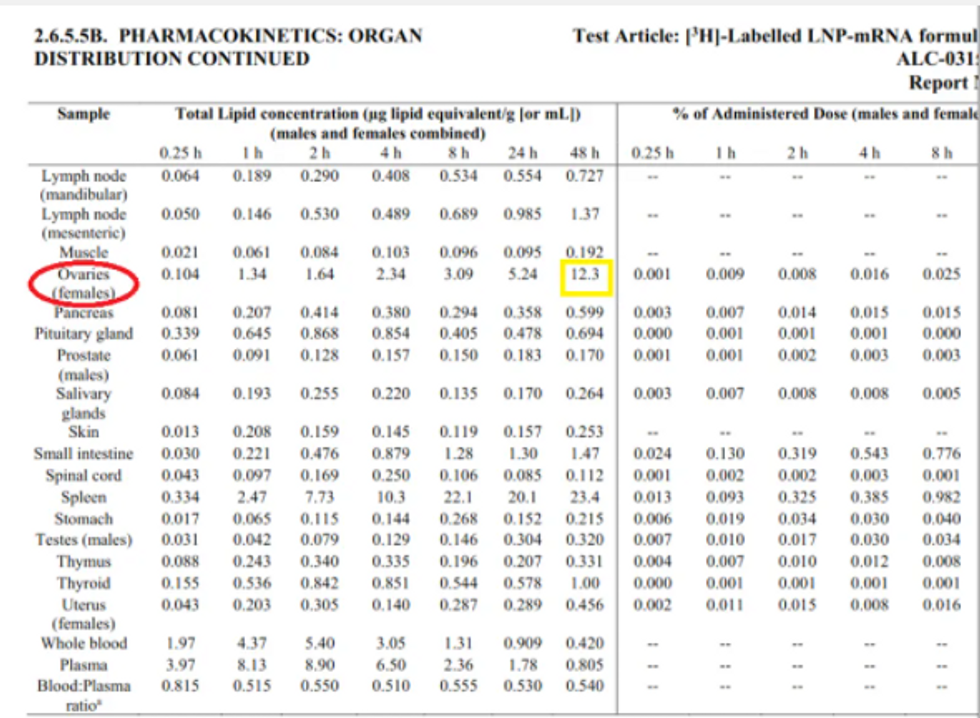
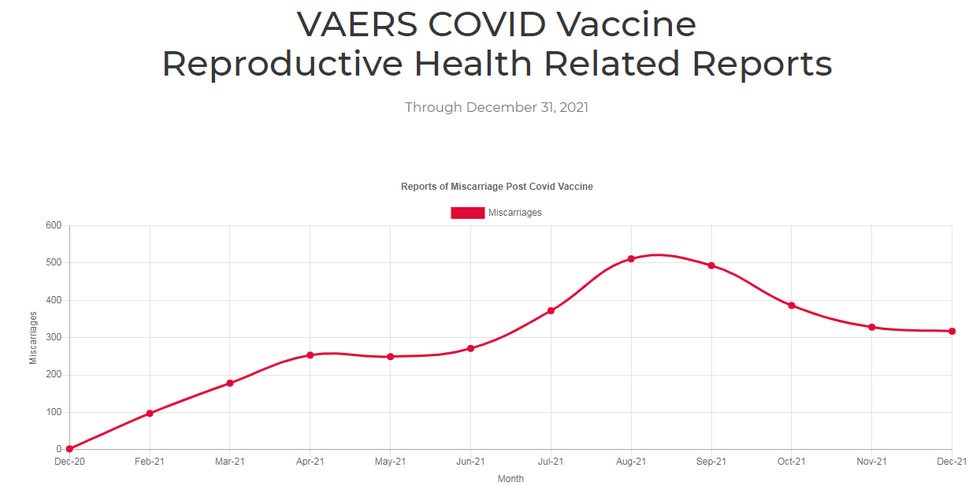
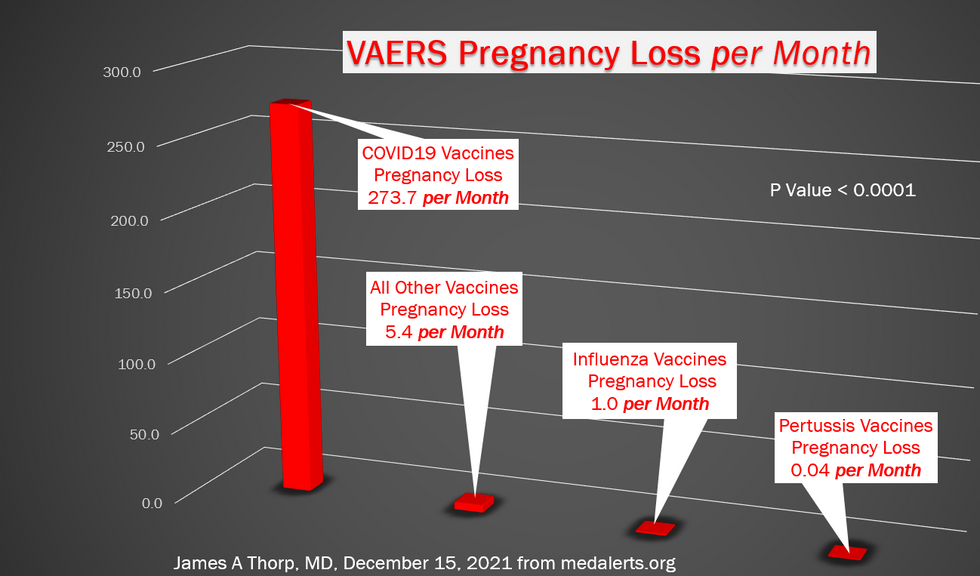
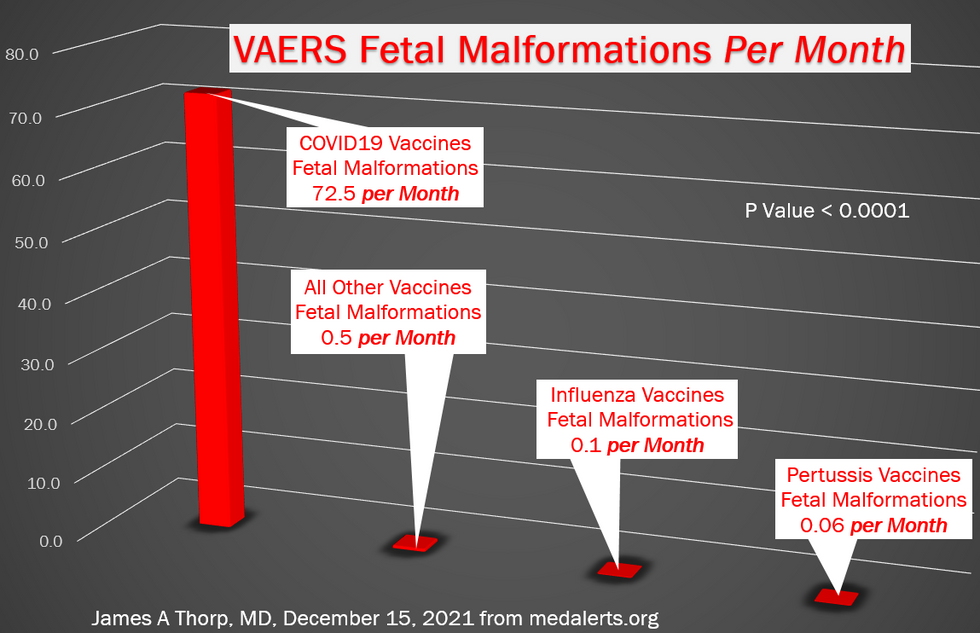
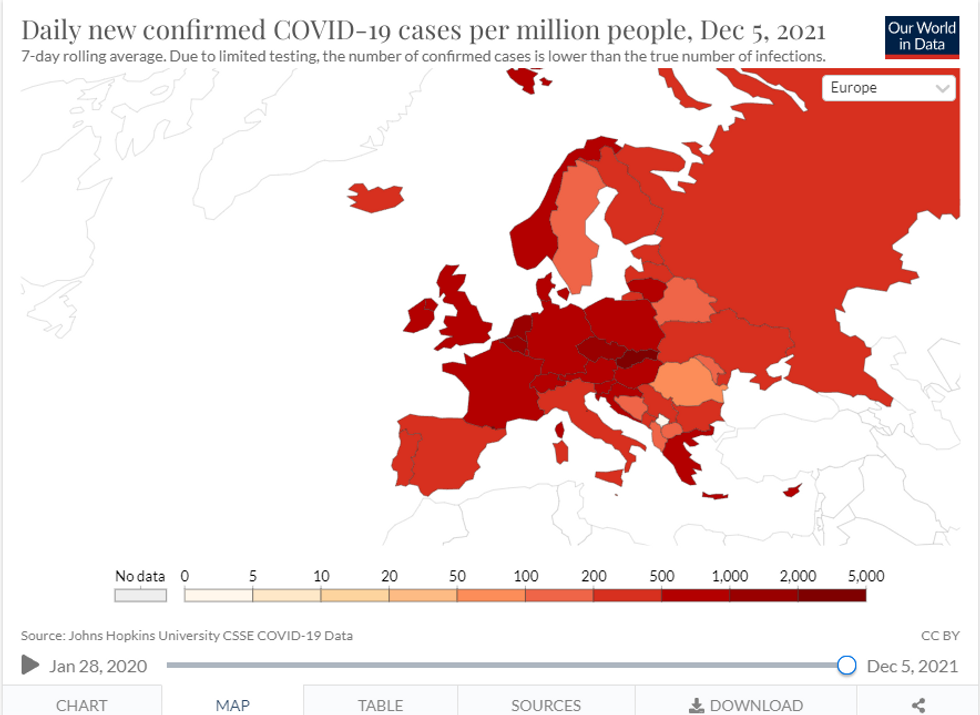
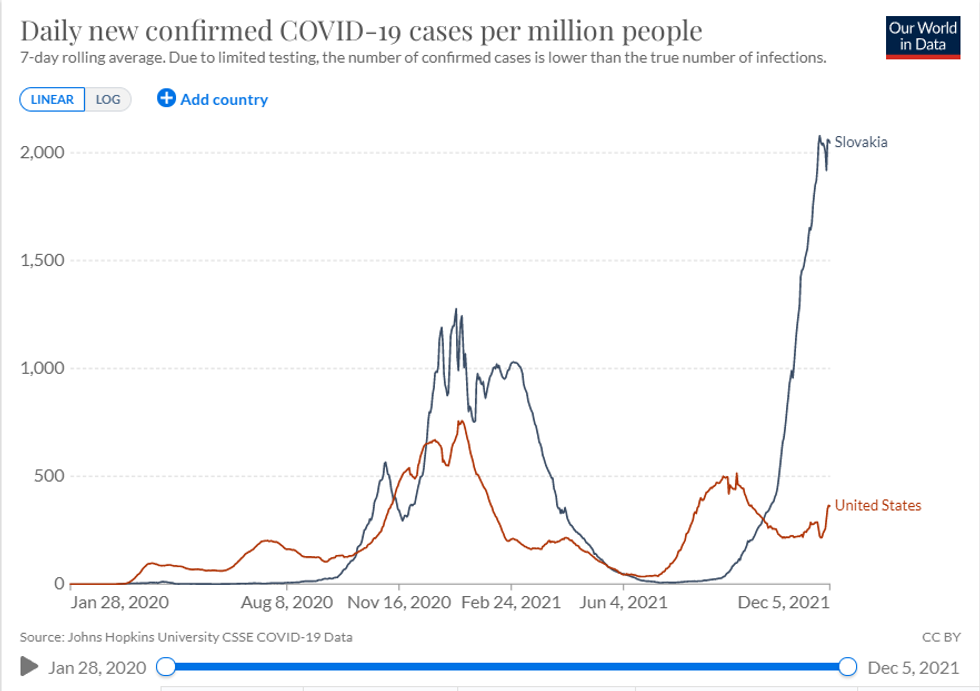


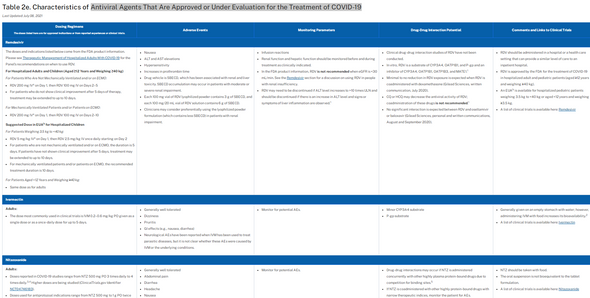
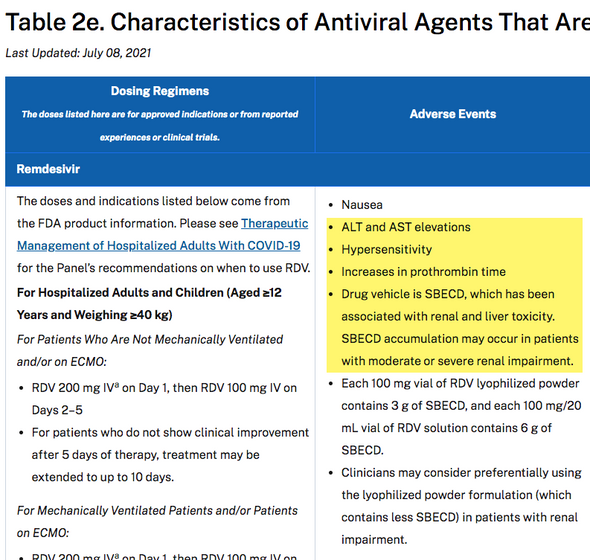
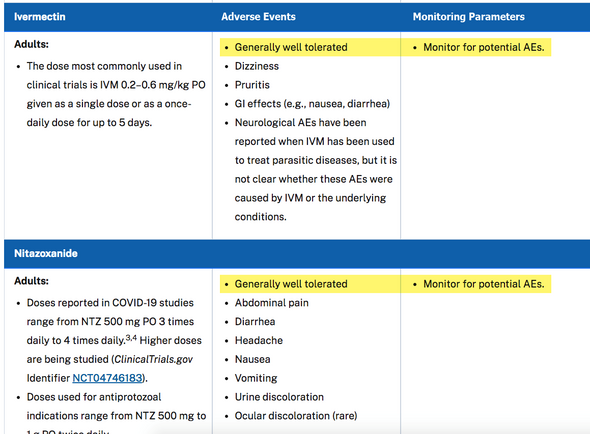
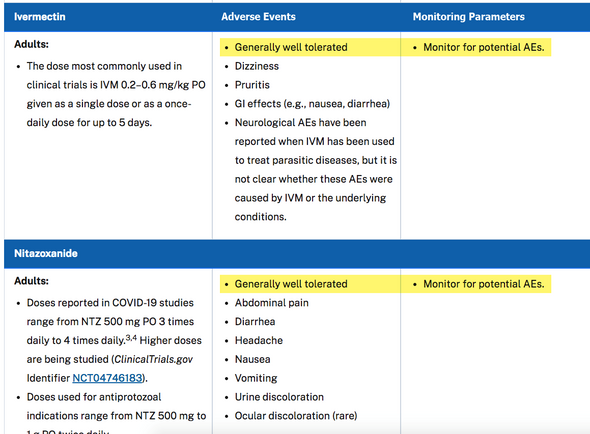






You must be logged in to post a comment.