Read more at https://www.theblaze.com/op-ed/cash-covid-and-coverup-part-4-the-virus-that-didn-t-bark/
Click here for part 1 of this series: Cash, COVID, and cover-up, part 1: The questions we should have asked of Fauci about the origins of COVID-19
Click here for part 2 of this series: Cash, COVID, and cover-up, part 2: The gain-of-function controversy
Click here for part 3 of this series: Cash, COVID, and cover-up, part 3: ‘You will have tasks today that must be done’
In the classic short story “The Adventure of Silver Blaze,” Sir Arthur Conan Doyle once famously had Sherlock Holmes solve a case based on what might be called the absence of a key piece of evidence. And while Holmes’ solution of the case might have been a bit of an unwarranted leap, sometimes the absence of evidence can be quite compelling, especially when it appears that evidence was likely destroyed. If a woman is found dead, and the next day her husband vanishes, leaving behind a house that has been scrubbed floor-to-ceiling with bleach, well … it doesn’t prove he murdered her, but pretty much everyone will have justified suspicions to that effect unless some compelling evidence surfaces to the contrary.
In examining whether the lab-leak theory is true or not, it is difficult to come to a hard and fast conclusion based on scientific evidence; however, that’s not because the science is in some way necessarily unclear. That’s because the Chinese government has gone to extraordinary lengths to destroy evidence and hamper any investigation into what happened at the Wuhan Institute of Virology in Wuhan, China.
That transparently obvious effort to cover up the truth is, in and of itself, a compelling piece of evidence.
++++++++++
Many years ago, the International Nucleotide Sequence Database Collaboration (INSDC) was created as a collaboration between the National Institutes of Health’s GenBank, the European Nucleotide Archive, and the DNA Databank of Japan. Information on the INSDC is available to the public as one of its foundational principles, which means that any person with access to the internet can find information about genetic sequences that have been uploaded to those databanks. In theory, this means virtually all genetic manipulations that have been the subject of any research project that has been published, since most scientific publications require genetic sequences to be deposited in the INSDC prior to publication.
The INSDC exists for several reasons, but one of the most important reasons is that if, say, an infectious disease pandemic breaks out somewhere in the world, scientists are supposed to be able to compare its genetic sequence to other known genetic sequences in order to quickly pinpoint the potential source of the virus; this information can help develop early treatments.
When the COVID-19 outbreak began, biologists began a similar search and did not find any likely candidates — until, that is, Shi Zhengli of the Wuhan Institute of Virology conveniently uploaded the sequence of a virus she called RaTG13 into GenBank on Jan. 23, 2020, shortly after the pandemic entered the public consciousness. RaTG13, as the story went, was collected from a cave in Yunnan province in 2013, and its genetic sequence matched the genetic sequence of SARS-CoV-2 by 96.3% — making it the first plausible natural ancestor to SARS-CoV-2.
The public opponents of the lab-leak theory latched on to RaTG13 as a savior. Here, at last, was a virus that had been found in the wild that was really quite close to SARS-CoV-2. The fact that it was miraculously unearthed just as the SARS-CoV-2 pandemic was gaining widespread global public attention in a laboratory that coincidentally was housed in the city where the pandemic began was apparently not a source of concern to these scientists. It was, for example, prominently referenced in what would become the seminal scientific article arguing for a natural origin of the pandemic, “The Proximal Origin of SARS-CoV-2.”
The immediate question that arises, given this sequence of events, is why, if RaTG13 was collected in May 2013 (as Shi claims), was it not uploaded to GenBank until after a pandemic caused by a virus that was so closely related to it began? Well, that is because China does not participate in the INSDC. The WIV, China’s first biosafety level 4 (BSL-4) facility, decided to keep genetic sequences discovered and/or created in their lab in its own proprietary database.
Implausibly, the United States government appears to have been OK with this arrangement and even approved taxpayer funding of research conducted in China that contained no guarantee that the United States would be provided with the results of that research, including the genetic sequences of viruses being studied.
Allow that to sink in for a moment: Your tax dollars were used to conduct research in a foreign country, with the express understanding that the foreign country was not obligated to even share the results of that research with the United States government, much less its public.
Well, you might be thinking, what’s so bad about allowing the Chinese government to maintain control over its own data? Surely we can just go to the WIV’s database and perform an additional search there?
As you may have already guessed, we cannot. The reason: The Wuhan Institute of Virology took its entire database offline.
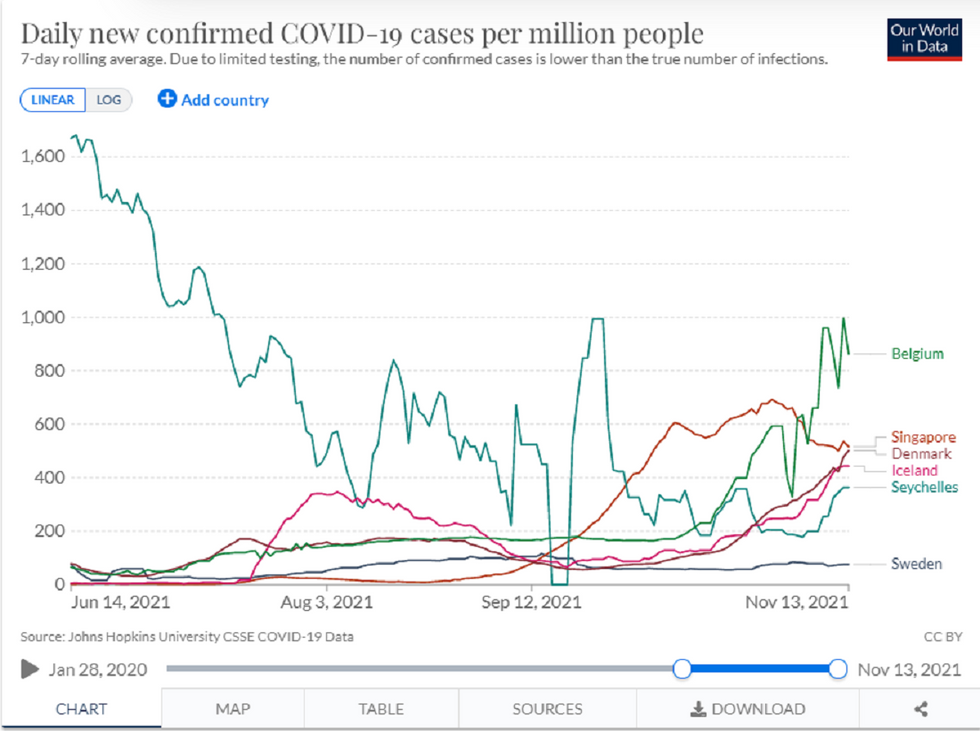
When, you might ask, did this event occur? In what is surely merely a spectacular coincidence, the WIV databases were pulled down on Sept. 12, 2019, which is probably a pretty good approximation of the actual date the first human was infected with SARS-CoV-2.
The Chinese government’s official story is that the WIV databases were pulled down because they were under attack by hackers. This might have been a plausible story, had the databases been pulled down after the pandemic became public knowledge and internet sleuths began aggressively investigating the Wuhan Institute of Virology. It is not a plausible story for why the databases had to be pulled down in September 2019, before anyone in the world had even heard of COVID-19 and before there was virtually any internet interest in the Wuhan Institute of Virology.
In a separate article published by researchers at the WIV, the WIV further claimed, perhaps by way of explanation as to why the genetic sequence of RaTG13 was unknown to the scientific community prior to the outbreak of the COVID-19 pandemic, that its scientists had never fully sequenced the virus before and only did so after the pandemic began, when they discovered that a “short region of RNA-dependent RNA polymerase (RdRp) from a bat coronavirus (BatCoV RaTG13) — which was previously detected in Rhinolophus affinis from Yunnan province — showed high sequence identity to 2019-nCoV.” According to the authors of this paper, who again worked at the WIV, at this point they finally “carried out full-length sequencing on this RNA sample,” whereupon it was uploaded to GenBank, thus showing that “the close phylogenetic relationship to RaTG13 provides evidence that 2019-nCoV may have originated in bats.”
Normal people, possessed of even a moderately healthy sense of skepticism, would have looked at this chain of events and concluded that the Chinese government obviously had something to hide. EcoHealth Alliance President Peter Daszak, on the other hand, who would repeatedly lambaste proponents of the lab-leak theory as crackpots and conspiracy theorists, apparently found nothing untoward in what was happening. In a London Times interview, he uncritically repeated Shi’s assertion that RaTG13 had been discovered while Chinese researchers were exploring a cave where six miners had died in a now-abandoned mine in Tongguan, whereupon they threw it in a freezer and forgot about it until 2020.
The “crackpots” and “conspiracy theorists” would soon be vindicated in their suspicions about the miraculous and entirely-too-convenient “discovery” of the supposedly thrown-in-a-freezer-and-forgotten RaTG13.
In the first place, DRASTIC sleuths began to notice that the genetic sequence to RaTG13 shared a curious affinity — a 100% affinity, in fact — with a partially revealed genetic sequence from a virus that was then called BtCOV/4991. DRASTIC members noted that not only were the two viruses genetically identical in the brief strip of BtCOV/4991 that had been published, but also the purported collection details of the virus were exactly the same. Faced with a growing paper trail, Shi would finally publicly admit in July 2020 that they were the same virus.
This admission made the entire purported origin story of RaTG13 a lie.
BtCOV/4991 was not collected and then thrown in a freezer and forgotten. It was, in fact, studied extensively by researchers in China, and its discovery and study was discussed in a 2016 paper published by Shi and her colleagues. It was mentioned again in a separate 2019 paper published by Shi and colleagues. Further, during the course of her admission that BtCOV/4991 and RaTG13 were the same virus, Shi made another startling admission: RaTG13 had, in fact, been fully sequenced in 2018, which indicates clearly that a) not only was RaTG13 not thrown in a freezer and forgotten, it was still being actively researched by the Wuhan Institute of Virology five years after its discovery, and b) it was not, as Shi’s colleagues had claimed, only fully sequenced after the pandemic began.
The official story of RaTG13 — that it was discovered in 2013 and then thrown in a freezer and forgotten until someone finally bothered to sequence it after the outbreak of COVID-19 — had now been exposed thoroughly as a lie, even by the concession of the people who originally made the claim. No one has yet been able to extract an answer from Shi or her colleagues as to why they falsely pretended that the full genetic sequence of RaTG13 was only discovered after the pandemic began, or why they pretended (by omission), for several months, that RaTG13 was a different virus from the BtCOV/4991 virus they had already extensively studied and written about.
Internet sleuths were quick to discover that many of the other claims made by Shi about RaTG13 were, at best, highly suspect. Recall that the specific event that precipitated the search of the Tongguan cave was that six miners who worked in the mine had died of a respiratory illness of uncertain etiology. Shi claimed in a March interview with Scientific American that the Tongguan miners had actually died due to a fungal infection they caught in the mine and that it was mere coincidence that during the exploration of the cave, they found RaTG13 — a clear attempt to downplay the lethality of RaTG13. However, DRASTIC member TheSeeker268 unearthed a master’s thesis by Chinese doctor Dr. Li Xu of Kunming Medical University, which clearly stated that the miner deaths were “caused by SARS-like CoV or bat SARS-like coronavirus that has been isolated from the Chinese rufous horseshoe bat.” The symptoms the miners died of were noted to be “identical to what we now call Covid-19.”
Furthermore, TheSeeker268 unearthed a 2016 thesis “written by Huang Canping, a student of Gao Fu, the current director of China CDC … In addition to what was already known, this document clearly states that WIV had tested the four miners (two had died by then); and all four of them had tested positive for SARS-like antibodies.”
Which raises the obvious question: Why would Shi lie and say that miners who died in the cave where the closest natural ancestor to SARS-CoV-2 was discovered actually died of a fungal infection?
+++++++++++
In addition to scrubbing the record of all genetic sequences researched at the WIV, and in addition to the demonstrably false statements from WIV researchers about their discovery of RaTG13, the Chinese government was working overtime in the early days of the pandemic to ruthlessly suppress any information about the pandemic from reaching the general public.
Dr. Li Wenliang, the ophthalmologist who first brought the attention of public awareness to the emerging pandemic, was pressured and threatened by Chinese authorities to recant his statement that the new coronavirus even existed and was infecting people. Li eventually allegedly caught COVID-19 himself and allegedly died from it in a Chinese hospital, despite his young age (34).
The Chinese government also engaged in a breathtaking campaign of internet and social media censorship designed to squash any internal debate — or even discussion — of the pandemic in China. The government campaign even reached into popular chatting app WeChat and livestreaming platform YY and included a shockingly broad list of terms, including, notably, a number of phrases that referenced the “Wuhan lab.”
These efforts were wrapped into China’s well-documented effort to censor and suppress negative coverage of its response to the pandemic as well — efforts that included the expulsion of American journalists and the disappearing of one of China’s most prominent citizens.
The importance of the disappearance of Ren Zhiqiang cannot be overstated in this story. While most Americans have likely never heard of him, he was, before his untimely disappearance, one of China’s most prominent private citizens, and he was involved in a very public criticism of China’s handling of the coronavirus pandemic. Imagine if, say, Dallas Mavericks owner Mark Cuban suddenly vanished from the face of the earth without a trace during the middle of a Twitter spat with then-President Donald Trump in March 2020, and no government agency seemed particularly interested in finding him, and no one who mattered even asked pointed questions of government officials as to whether they were involved in his departure.
Almost no one believes that Ren is not either dead or imprisoned at the hands of the communist Chinese government at this point, and the Chinese government does not seem particularly interested in combating that perception publicly. Imagine the impression such an event would make upon the average Chinese citizen — or, for that matter, any researcher at the Wuhan Institute of Virology who might feel tempted to contradict the government line about what happened in that laboratory.
++++++++++++
If the censorship campaign the Chinese government conducted against its own citizens was thorough, it was nothing compared to what the Chinese government would do to the international community. From the onset of the pandemic in early 2020, China lied, hid information, and stonewalled World Health Organization researchers as they attempted to learn about the virus.
Publicly, both sides acted as if everyone was getting along. Chinese authorities told WHO Director-General Tedros Adhanom Ghebreyesus in a Jan. 25, 2020 letter they would welcome international experts to China to help “strengthen epidemic prevention and control.” Tedros met with President Xi Jinping in Beijing on Jan. 28 and praised the Chinese for their openness and transparency. In reality, as the Associated Press would report, China frustrated WHO officials by delaying the release of information, and Tedros and others were only lauding China in public “because they wanted to coax more information out of the government.”
In early January, three different Chinese labs had fully decoded the genetic sequence of SARS-CoV-2, but instead of sharing that information with the world, China sat on it. The virus was first decoded on Jan. 2, but it wasn’t until after the Wall Street Journal reported that Chinese scientists had discovered a new coronavirus on Jan. 8, a week later, that Chinese state media announced the discovery of the new coronavirus. China did not include any information about its genome, diagnostic tests, or detailed patient data that would have given scientists a clue about how infectious the disease was.
There was also a two-week period when Chinese officials censored reports of new infections in Wuhan. Operating under the belief that infections weren’t spreading, Chinese researchers, unaware of the censorship, told WHO officials that the virus didn’t transmit easily between humans. This led the WHO on Jan. 5 to announce that based on preliminary data from China, there was no evidence of significant transmission between humans and no need for travelers to take precautions. Of course, once the genetic sequence of the virus was made public and it turned out the virus was highly contagious, the WHO was made to look “doubly, incredibly stupid” for downplaying the virus, in the words of Dr. Tom Grein, chief of the WHO’s acute events management team.
Meanwhile, people began getting sick with COVID-19 throughout the region. When one woman fell ill in Thailand on Jan. 8, researchers attempted to match the virus to illnesses that had been reported in China, but the Chinese authorities hadn’t yet published the viral sequences. China’s obfuscation of data about COVID-19 prevented countries from taking steps to mitigate spread early in the pandemic, resulting in people getting sick and dying.
The SARS-CoV-2 sequence wasn’t published until Jan. 11, when a team led by Chinese virologist Zhang Yongzhen angered Chinese authorities by uploading the virus to virological.org. The next day, Zhang’s lab was temporarily shut down. But now that the viral sequence was out there, the Chinese CDC, Wuhan Institute of Virology, and Chinese Academy of Medical Sciences each published their viral sequences for SARS-CoV-2 to GISAID, a platform for scientists to share data on viruses. The WHO’s first investigative team arrived in Wuhan on Jan. 14. One of the team’s tasks was to visit the Huanan Seafood Market, where scientists believed the virus’ first major outbreak took place, but from the beginning there was uncertainty about where Chinese authorities would allow the researchers to go and who they would be permitted to talk to. China had strongly opposed an independent investigation that it could not fully control, and before the terms of the investigation were agreed to, the WHO complained that China was taking too long to finalize arrangements for the investigators.
But after senior WHO delegation met with Chinese officials in Beijing on Jan. 28, Tedros made no public mention of China’s obstruction in the hope that the Chinese would be more forthcoming in the future. On Jan. 30, the WHO declared the outbreak to be a public health emergency of global concern. In the following months, WHO researchers continued to work with Chinese and on March 11, 2020 WHO declared COVID-19 could be characterized as a pandemic.
In May, the 73rd World Health Assembly charged WHO Director-General Tedros to form an international investigative team “to identify the zoonotic source of the virus and the route of introduction to the human population.” But even the vote on this resolution was delayed as Chinese officials “were negotiating over every comma,” as one former U.S. official described to the Wall Street Journal.
Chinese officials continued to play hardball with the WHO until in July 2020 an agreement was reached for a “terms and references” document that stated the goals of the investigation, was silent on the lab-leak theory, and gave China veto power over who would be on the WHO team.
The WHO investigative commission that eventually formed was fatally flawed by the prominent inclusion of one Peter Daszak in its ranks.
Daszak, by way of reminder, had been literally the global and public ringleader of the group of scientists who had been publicly ridiculing lab-leak theory proponents and attempting to quash public discussion of their theory for over a year. He was also the president of an organization that had for years funneled significant amounts of money to the lab he was purporting to investigate and that had widely publicized its frequent collaboration with that lab — meaning that if the lab-leak theory were true, he would be one of the first people in the public hot seat.
Sending Daszak as part of the team was grossly inappropriate not only because of the obvious conflicts of interest he was subject to, but also because, even in the absence of those conflicts of interests, Daszak had publicly and loudly made up his mind about the subject of the investigation before it even began.
Daszak was, in fact, the only scientist from the United States who was part of the WHO’s investigative team.
However, that did not stop the Chinese from stonewalling anyway. On Jan. 5 2021, some members of the Team began their journey to China, only for Chinese officials to deny the WHO team entry into the country for several days until Jan. 14.
After two weeks of quarantine, the WHO investigation proceeded under severe restrictions. According to the Wall Street Journal, the team was restricted to one part of their hotel by quarantine rules, forced to eat separately from their Chinese partners, and had limited contact with anyone outside the team. They proceeded to take a propaganda tour visiting the hospital where Beijing claims the first COVID-19 case was officially reported, another hospital where they visited an exhibition commemorating President Xi’s leadership, and cold-storage facilities at the Huanan market where Chinese officials claim the virus entered China from abroad.
Accounts from team members reported by the Journal indicate Chinese authorities refused to share raw data with the investigators, instead handing over their own data analysis. Even the team’s visit to the Wuhan Institute of Virology was limited to only three hours.
Nevertheless, the WHO released a report in February 2021 that determined it was “extremely unlikely” that COVID-19 leaked from a lab, determining instead that the most likely origin of the virus was a zoonotic event — a bat virus transmitting to another animal carrier and then leaping to humans sometime toward the end of 2019. Part of the investigation included inspecting the Wuhan Institute of Virology’s lab, under Chinese supervision, and WHO team leader Peter Ben Embarek said that the safety protocols at the lab led them to conclude “it was very unlikely that anything could escape from such a place.”
But the WHO investigation has since been highly criticized. On March 2, 2021, two dozen experts, including virologists, signed an open letter that called for a new international investigation on the origins of COVID-19. They said that the WHO did not have the independence or access “to carry out a full and unrestricted investigation” into the lab-leak theory. During a “60 Minutes” interview in March, Jamie Metzl, an advisory board member for WHO and one of the letter’s signatories, said the WHO team “didn’t demand access to the records and samples and key personnel” while they visited the Wuhan Institute of Virology. He blamed China for denying the investigators access to those materials. Metzl further said that the WHO agreed to let China do the “primary investigation” into the origins of the virus and then share its findings with the team.
Daszak’s inclusion on the team, in particular, led to entirely predictable results.
Speaking to “60 Minutes,” Daszak more or less confirmed that the WHO team’s investigative process, when it came to the Wuhan lab, was to just ask the lab staff questions and take their answers at face value.
“We met with them,” Daszak told Lesley Stahl. “We said, ‘Do you audit the lab?’ And they said, ‘Annually.’ ‘Did it you audit it after the outbreak?’ ‘Yes.’ ‘Was anything found?’ ‘No.’ ‘Do you test your staff?’ ‘Yes.’ No one was —”
“But you’re just taking their word for it,” interjected Stahl.
“Well, what else can we do?” Daszak replied.
Incredibly, he argued that the answers the WHO team received from China were “correct and convincing,” even though Chinese authorities had demonstrably worked to suppress information about the virus.
When Stahl pointed out how China had “engaged in a cover-up,” Daszak was dismissive.
“Well, that wasn’t our task to find out if China had covered up the origin issue,” he said.
That jaw-dropping assertion was certainly a surprise to the rest of the world, which was told by the WHO that that was exactly what the purpose of their investigation was, and to Daszak’s fellow investigators, who were charged with going to China to “better understand the origins of the virus,” according to the terms of the report they prepared.
Only someone as thoroughly dedicated to the proposition that there was no chance China could have been in any way dishonest as Daszak could have concluded from such a charge that actually checking out any of the statements made by Chinese scientists was not part of the scope of work. It was as if, seeking to investigate the disappearances of Nicole Brown Simpson and Ronald Goldman, the WHO had sent a spokesperson for O.J. Simpson as their lead investigator and was surprised to learn that he didn’t feel like it was his job to question O.J.’s denials.
Governments weren’t happy either. In a joint statement, the United States and 13 other countries raised concerns that China had refused to provide investigators with “complete, original data and samples. Additionally, in apparent contradiction of his own organization’s findings, WHO Director-General Tedros acknowledged on March 30 that “all hypotheses remain on the table,” as to the origins of the virus.
In remarks to WHO member states, Tedros said, “Further data and studies will be needed to reach more robust conclusions.” He called on China to be more forthcoming with data in the future.
China reacted by denying that it hid data from WHO investigators. It accused the West of politicizing the report. At the same time, the Chinese government has shared disinformation and conspiracy theories about COVID-19 being engineered as a bioweapon in the U.S. and brought to China by the U.S. military.
In July 2021, China rejected WHO requests for a renewed investigation in China, asserting that such investigations should be conducted elsewhere. Chinese authorities have also deflected responsibility for COVID-19 by claiming the virus was brought to China via frozen food packaging.
On July 22, Vice Health Minister of the National Health Commission Zeng Yixin slammed the door shut on a second investigation by denouncing the WHO’s request as “arrogant” and “shocking.”
“In some aspects, the WHO’s plan for next phase of investigation of the coronavirus origin doesn’t respect common sense, and it’s against science. It’s impossible for us to accept such a plan,” said Yixin.
With official investigations now thoroughly blocked by China, independent investigations have proceeded but with extremely limited success. The medical journal The Lancet established an international task force to investigate the origins and spread of COVID-19 in November 2020. But the task force was led by Daszak, who in June 2021 was forced to recuse himself after his connections to the Wuhan Institute of Virology and potential conflicts of interest became widespread knowledge.
In June 2021, an American scientist discovered evidence that Chinese researchers deleted SARS-CoV-2 viral sequences from the National Institutes of Health’s Sequence Read Archive (SRA). NIH later confirmed that after Chinese scientists submitted the data in March 2020, they were “requested to be withdrawn” three months later in June. On July 5, 2021, the missing viral sequences reappeared in a database controlled by Chinese authorities. Chinese authorities claimed that the viral sequences were removed and later reuploaded elsewhere to correct a copy-editing error.
The Chinese researchers have not explained why they didn’t mention the copy-editing error when they requested that the NIH take down their sequences, nor why they waited for a year before uploading them to another database. The bottom line, as this episode demonstrated, is that any investigation into COVID-19’s origins remains at the mercy of China’s willingness to be open and transparent — which they are not.
+++++++
What, then, are we to make of the actual scientific evidence about what the virus looks like?
In the absence of being able to access honest records at the WIV, which will likely never happen, or thoroughly examine its lab personnel, which will also likely never happen, the honest answer is: not much.
Scientific opponents of the lab-leak theory have expended a tremendous amount of energy arguing that the genetic features of the virus are consistent with natural evolutionary mutations and that there are no sequences that evince evidence of being an obvious man-made creation. We cannot cast doubt on the veracity of those conclusions, but they are, essentially an argument against a straw man. Very few people have suggested that the virus was specifically engineered as a bioweapon, and even if it was engineered as a bioweapon, surely the Chinese would have taken care to make it look natural.
It ignores, furthermore, two facts that are central to the discussion of this issue.
First, the work undertaken at the WIV (that we know about) specifically involved the creation of chimeric viruses that were intended to mimic possible evolutionary processes. Recall what the ostensible purpose of gain-of-function research is, which is to develop treatments and/or vaccines for viruses that might occur naturally.
Members of the media, who relied on the group of scientists who confidently declared the lab-leak theory a baseless conspiracy theory (most of whom have now backtracked) have assumed that scientists are somehow able to determine that a virus is engineered merely by looking at its genetic structure, as if the process of creating a chimeric virus leaves behind some irrefutable fingerprint, and that in the absence of such a fingerprint, a virus is obviously naturally occurring. That is not how it works.
Although it would certainly be possible to engineer a virus that has characteristics that would be obviously artificial, It is also entirely possible — in fact, it is what people like Ralph Baric have spent the entirety of their professional lives learning to do — to artificially engineer a virus that looks for all the world like a virus that might have evolved naturally. Recall that a central purpose of the gain-of-function research community is to develop vaccines and/or treatments for diseases that don’t yet exist but have a reasonable probability of someday existing in the future. One does not accomplish such a goal by generating viruses that could not possibly be produced by natural evolution.
Every virus created by Shi or Baric in a lab is one that, if you didn’t have access to a research paper telling you they created it, you would look at and say, “Well, this looks like a virus that might have arisen through natural evolutionary processes.” That is the entire point of what these researchers were doing. So pointing out that the viruses don’t look obviously artificial, as has repeatedly been done, is no answer at all, and anyone who confidently tells you that they can tell a virus wasn’t engineered just by looking at it is selling something. We have no way of knowing, as just one example, that RaTG13 itself was not engineered, except to take Shi’s word for it about where she found it. We can’t even verify that it hasn’t been substantially modified since she found it, since the genetic records have been intentionally erased.
One thing that would help us definitively rule out the possibility of a lab leak would be the discovery of an intermediate host, either animal or human, but no such host has yet come forward. These hosts have been found with other respiratory outbreaks, but none have yet come forth for SARS-CoV-2, in spite of the fact that Chinese researchers have, as previously noted, been assiduously collecting and cataloguing samples from bats for years.
The initial prime suspect for intermediate host was the poor pangolin, a kind of anteater that is found in China, based upon the fact that the receptor binding motif (RBM) of SARS-CoV-2 bears striking similarities to SARS strains that have been found in pangolins. Additionally, pangolins were found to be infected with other coronaviruses that were reasonably similar to SARS-CoV-2; however, no pangolins have yet been found to be infected with a virus that could plausibly serve as the actual ancestor to SARS-CoV-2, even though early papers touting a natural origin for the virus heavily promoted the theory that pangolins had served as an intermediate host for the virus between bats and humans.
It also might have helped shed light on the situation if researchers had been permitted to investigate laboratory staff early on in the pandemic, but the Chinese government refused.
The fact of the matter is, as an international group of respected scientists recently wrote in The Lancet, “There is so far no scientifically validated evidence that directly supports a natural origin.”
These scientists challenged the arguments put forward in the “Proximal Origins” letter and elsewhere that ruled out the possibility of the lab-leak theory by showing how proponents of the natural origins explanation fell for a logical fallacy (edited for readability):
The question of the proximal origin of SARS-CoV-2—ie, the final virus and host before passage to humans—was expressly addressed in only one highly cited opinion piece, which supports the natural origin hypothesis, but suffers from a logical fallacy: it opposes two hypotheses—laboratory engineering versus zoonosis—wrongly implying that there are no other possible scenarios.
The article then provides arguments against the laboratory engineering hypothesis, which are not conclusive for the following reasons. First, it assumes that the optimisation of the receptor binding domain for human ACE2 requires prior knowledge of the adaptive mutations, whereas selection in cell culture or animal models would lead to the same effect. Second, the absence of traces of reverse-engineering systems does not preclude genome editing, which is performed with so-called seamless techniques.
Finally, the absence of a previously known backbone is not a proof, since researchers can work for several years on viruses before publishing their full genome (this was the case for RaTG13, the closest known virus, which was collected in 2013 and published in 2020).
Based on these indirect and questionable arguments, the authors conclude in favour of a natural proximal origin. In the last part of the article, they briefly evoke selection during passage (ie, experiments aiming to test the capacity of a virus to infect cell cultures or model animals) and acknowledge the documented cases of laboratory escapes of SARS-CoV, but they dismiss this scenario, based on the argument that the strong similarity between receptor binding domains of SARS-CoV-2 and pangolins provides a more parsimonious explanation of the specific mutations. However, the pangolin hypothesis has since been abandoned so the whole reasoning should be re-evaluated.
The main point they advance in their letter is that both the lab-leak and natural origins hypotheses remain viable, because we don’t have all the evidence, and both should be encouraged as a matter of open and honest public debate.
All that having been said, there are features of SARS-CoV-2 that are, in fact, similar to chimeric viruses that have been created in a lab. DRASTIC member Yuri Deigin catalogued some of those similarities at great length in a fascinating Medium post in April 2020. Specifically, Deigin noted that the virus looked like a virus that was “based on the ancestral bat strain RaTG13, in which the receptor binding motif (RBM) in its spike protein is replaced by the RBM from a pangolin strain, and in addition, a small but very special stretch of 4 amino acids is inserted, which creates a furin cleavage site that, as virologists have previously established, significantly expands the “repertoire” of the virus in terms of whose cells it can penetrate.”
Deigin, whose work is worth reading in full, was careful to emphasize that such a chimeric mutation could have occurred in nature. However, creating just such a kind of virus was also consistent with the exact sort of work Shi, with the help of Baric, had performed in the past:
Indeed, virologists, including the leader of coronavirus research at the Wuhan Institute of Virology, Shi Zhengli, have done many similar things in the past — both replacing the RBM in one type of virus by an RBM from another, or adding a new furin site that can provide a species-specific coronavirus with an ability to start using the same receptor (e.g. ACE2) in other species. In fact, Shi Zhengli’s group was creating chimeric constructs as far back as 2007 and as recently as 2017, when they created a whole of 8 new chimeric coronaviruses with various RBMs. In 2019 such work was in full swing, as WIV was part of a $3.7 million NIH grant titled Understanding the Risk of Bat Coronavirus Emergence. Under its auspices, Shi Zhengli co-authored a 2019 paper that called for continued research into synthetic viruses and testing them in vitro and in vivo.
Further information that has come to light since Deigin’s work has further solidified the fact that Shi, with the help of Daszak, Baric, and others, were seeking funding for the creation of a chimeric bat coronavirus that would behave in ways eerily similar to SARS-CoV-2. As we have reported previously, in 2018, Daszak’s EcoHealth Alliance sought $14 million in funding from DARPA for a collaborative project between Baric, Shi, and others that would “synthesize spike glycoproteins which bind to human cell receptors and insert them into SARSr-CoV backbones to assess whether they can cause SARS-like disease.”
Even more specifically, the project’s goal stated that it intended to release “enhanced airborne coronaviruses” into Chinese bat populations in order to inoculate them against diseases that could spread to humans. Although DARPA ultimately refused to fund the proposed Daszak project, deeming it too risky, neither Daszak nor Baric returned a request for comment as to whether the research continued with alternate funding. Certainly, there is no way to determine whether Shi and her fellow WIV researchers undertook the project on their own and simply used funding from the Chinese government to do so. If they had, the end result of such a project would have looked a lot like SARS-CoV-2.
At the end of the day, it may now be impossible to scientifically prove the truth or falsity of the lab-leak theory. But that isn’t by accident: It’s because the Chinese government undertook an extensive, obvious, and thorough effort to destroy and restrict access to evidence that was necessary to conduct a full and thorough investigation. The conclusion you draw from that is, of course, up to you.
And if it is impossible to tell with any certainty now that the virus didn’t escape from the WIV, it was definitely impossible to rule the possibility out with certainty in the early months of 2020.
Which raises the somewhat important question: Why did scientists like Peter Daszak, et al., pretend that it was?
Editor’s note: This article was updated on Sept. 27, 2021 with additional information about the WHO joint investigative team.




































































You must be logged in to post a comment.