Robert F. Kennedy, Jr., on Monday said former President Donald Trump had promised him “control” over key public health and agriculture agencies if Trump wins the election next week. During a virtual event, Kennedy said, “the key that President Trump has promised me is control of the public health agencies, which are [Health and Human Services] and its sub-agencies, CDC, FDA, NIH, and a few others … and then also the [Department of Agriculture],”Politico reports.
Kennedy didn’t specify a particular role, such as HHS Secretary, which would likely require Senate confirmation, an outcome that could be challenging due to Kennedy’s outspoken vaccine skepticism. However, it’s possible he could influence health policy in an advisory role if an official appointment isn’t viable.
The Trump campaign has not denied Kennedy’s claims, but they call discussions about appointments “premature.” Trump’s national press secretary added that Trump wants to collaborate with “passionate voices” like Kennedy to improve food safety and fight chronic illnesses affecting children.
Trump himself suggested at his Madison Square Garden rally Sunday that he’d let Kennedy “go wild” on reforming food and medicine policies if re-elected.
Kennedy, who suspended his own presidential campaign in August and endorsed Trump, serves on the former president’s transition team.
He has been campaigning for him in crucial swing states since dropping out of the race. Kennedy is founder of Children’s Health Defense, a non-profit organization aimed at “ending childhood health epidemics by eliminating toxic exposure,” according to its website.
Protesters march Aug. 3 in London in the wake of Dr. Hilary Cass’ warning about the harms of so-called gender-affirming care. A newly revealed email shows a U.S. health official supports “puberty blockers” while admitting they increase the risk of suicide. (Matthew Chattle/Future Publishing/Getty Images)
FIRST ON THE DAILY SIGNAL—Former officials in the U.S. Department of Health and Human Services and the Food and Drug Administration condemned what they described as the FDA’s duplicity in allowing off-label use of so-called puberty blockers while loudly condemning the use of far safer drugs to treat COVID-19.
“During the Trump administration, the media falsely accused us daily of ‘politicizing America’s public health agencies.’ Yet the same media is now silent on [Vice President Kamala] Harris and [President Joe] Biden’s FDA’s anti-science, purely political insanity,” Brian Harrison, former chief of staff at HHS and now a member of the Texas House of Representatives, told The Daily Signal in a written statement.
“We’ve now learned that the same FDA that banned mothers from importing safe formula for starving babies and kept safe COVID treatments from patients was apparently pushing dangerous puberty blockers for kids,” Harrison added.
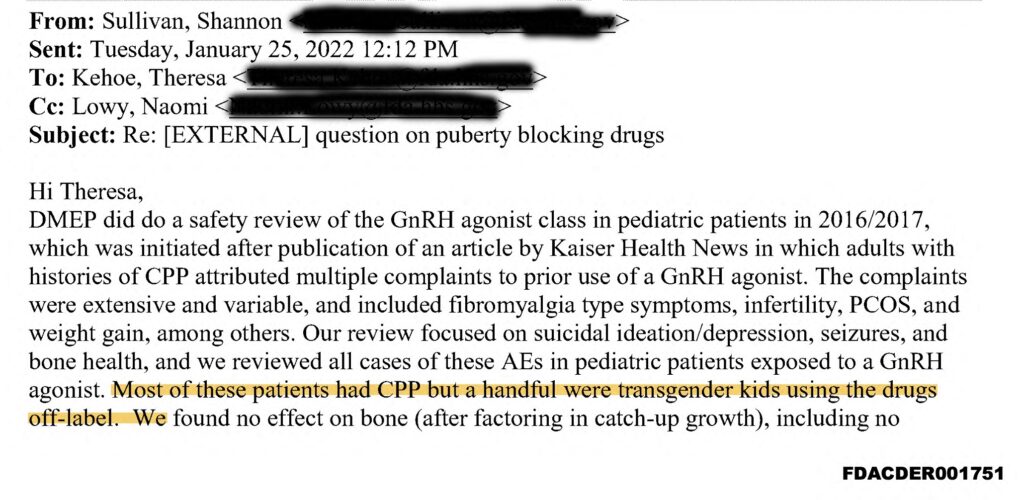
In the Jan. 25, 2022, email, Shannon Sullivan, clinical team leader at the FDA’s Division of General Endocrinology, noted that the agency’s Division of Metabolism and Endocrinology Products performed a “safety review of the GnRH agonist class in pediatric patients in 2016/2017.”
GnRH stands for “Gonadatropin-releasing hormone.” GnRH agonists prevent the natural release of testosterone and estrogen that initiate puberty.
“Our review focused on suicidal ideation/depression, seizures, and bone health,” Sullivan wrote in the 2022 email. Although most of the minors in the study suffered from central precocious puberty (in which puberty starts too early), she said, “a handful were transgender kids using the drugs off-label.”
“We found no effect on bone (after factoring in catch-up growth), including no increase in fracture risk,” she noted. “We did find increased risk of depression and suicidality, as well as increased seizure risk and we issued [safety-related labeling changes].”
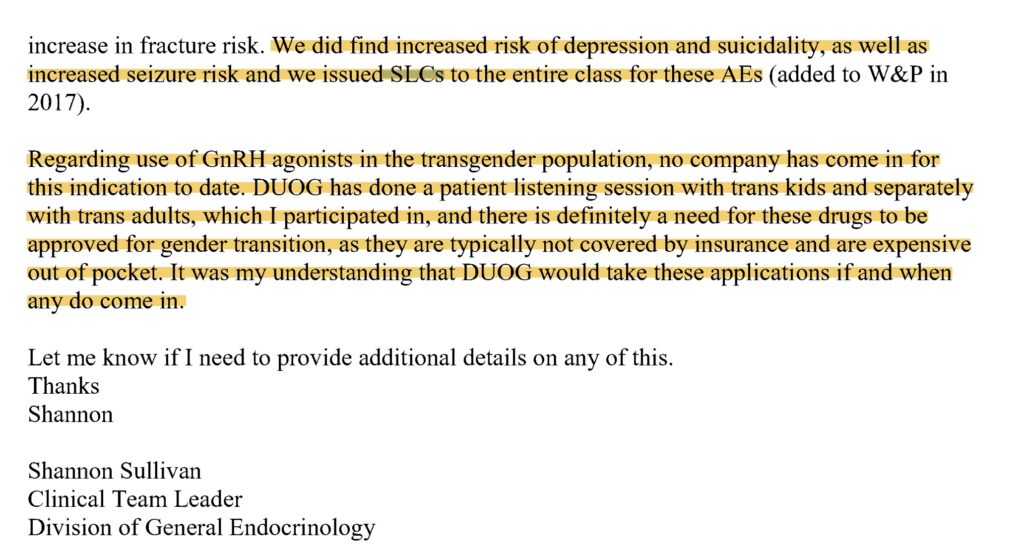
Yet, as The Daily Signal reported, Sullivan went on to recommend approving GnRH agonists for minors.
The FDA’s Division of Urology, Obstetrics, and Gynecology, she wrote, “has done a patient listening session with trans kids and separately with trans adults, which I participated in, and there is definitely a need for these drugs to be approved for gender transition, as they are typically not covered by insurance and are expensive out of pocket.”
Sullivan also said that “no company has come in” to provide “GnRH agonists in the transgender population” yet. However, she added, “it was my understanding” that the FDA division “would take these applications if and when they do come in.”
Screenshot
Transgender activists claim that minors who identify with the gender opposite their biological sex need experimental medical alterations such as GnRH agonists either to prevent puberty or to force their bodies to resemble the bodies of the opposite sex. Activists mask the nature of these interventions with the term “gender-affirming care” and insist that without these interventions, kids will commit suicide.
Roger Severino, former director of the Office of Civil Rights at HHS and now vice president of domestic policy at The Heritage Foundation, emphasized the contradiction between the rhetoric supporting “gender-affirming care” and the findings noted by the FDA’s Sullivan.
“HHS still claims puberty blockers for 12-year-olds are fully ‘reversible,’ seemingly oblivious to the fact that suicide is as irreversible as it gets,” Severino quipped.
FDA’s Duplicity on COVID-19, ‘Puberty Blockers’
David Gortler, a Yale University-trained pharmacologist who previously was a senior adviser to the FDA commissioner on policy and drug safety, raised the alarm about GnRH agonists for minors. Gortler told The Daily Signal that the Food and Drug Administration is being “duplicitous” in how it uses its Adverse Event Reporting System (AERS), a database of reactions to certain drugs that users report to the FDA.
The FDA relied heavily on the reporting system’s data to declare that hydroxychloroquine was unsafe after finding only a few hundred reports of adverse events, he said, but the agency dismisses a considerably higher number of such reports for GnRH agonists.
“GnRH agonists account for 70,000 adverse reports,” Gortler said. “While these reports still need to be reviewed, it is a remarkable number of adverse events for what should be a niche, otherwise rarely clinically indicated, class of drugs.”
Yet the FDA often dismisses these reports as “not confirmed”; “not establishing causation”; “no definitive proof”; and “not establishing a rate of occurrence.”
Gortler, who has analyzed the data himself, showed that preliminary analysis to The Daily Signal. According to his analysis, AERS reports 70,000 adverse reactions to GnRH agonists, 2,510 of them involving children aged 14 or younger.
Adverse reactions include hallucinations, bone disorders, cardiac arrest, abdominal pain, migraine, mood alterations, a clot in the heart, pelvic pain, seizures, abnormal skin odor, blindness, and more. Among patients ages 4 to 13, a total of 21 had thoughts of suicide.
The AERS database includes 30 records noting the death of a patient between the ages of zero and 14 where a “puberty blocker” is the primary suspect drug.
These cases include a 10-year-old who died of a hemorrhagic stroke after taking Lupron, a brand of synthetic hormone, in March 2014; a 5-year-old who died of cancer reported in May 2022; an 8-year-old who died of liver failure after receiving leuprolide acetate, a synthetic drug, in March 2004; and a 14-year-old who “completed suicide” in April 2017.
“Even though this drug is objectively unsafe, they seem to be selectively turning a blind eye to it, seemingly in sync with White House messaging,” Gortler said, referring to FDA officials.
“At the same time,” he added, “the FDA selectively heavily involved itself in the off-label administration of ivermectin and hydroxychloroquine, both of which were relatively much safer than GnRH agonists, based on clinical studies, randomized controlled trials, AERS reports, plus other epidemiological findings.”
Where Do ‘Puberty Blockers’ Come From?
The former FDA adviser also told The Daily Signal that physicians developed GnRH agonists to help treat certain cancers that depend on estrogen or testosterone. Removing estrogen and testosterone from cancer patients to prolong their lives makes sense, Gortler said, because it prevents the progress of an invasive, malignant disease. But giving these drugs to physiologically and genetically healthy kids is a completely different story, he said.
“This drug was tested, designed, and FDA-approved for use in an older, cancer-afflicted population,” Gortler said.
“The human body has around 100 trillion cells,” Gortler noted. “High school biology taught us that in each of those nucleated cells, there are either XX or XY chromosomes denoting a female or male sex, respectively. No drug or medical procedure will ever be able to fight 100 or so trillion cells and trying to do so would be a fool’s errand.”
He compared “puberty blockers” to the outdated, dangerous custom of Chinese foot binding, in which a young girl’s feet would be tightly wrapped to keep them from growing naturally.
“Similarly, GnRH agonists block a normal, healthy development process from occurring,” Gortler said. “Just because it’s not something that isn’t directly and obviously visible doesn’t mean that it’s any less clinically, scientifically, or ethically dangerous.”
The FDA did not respond to The Daily Signal’s request for comment.
The Elon Musk-founded Neuralink, the medical device company developing implantable brain-computer interface microchips, has received U.S. Food and Drug Administration approval to start human clinical trials as early as this summer.
The company announced what it calls “an important first step” last Thursday and expects to share more information on recruitment for the clinical trial in the near future.
“We are excited to share that we have received the FDA’s approval to launch our first-in-human clinical study!” the company tweeted. “This is the result of incredible work by the Neuralink team in close collaboration with the FDA and represents an important first step that will one day allow our technology to help many people. Recruitment is not yet open for our clinical trial. We’ll announce more information on this soon!”
While details are still scant, the trial is expected to focus on Neuralink’s brain-computer interface (BCI), a Class III medical device that connects the brain to an external computer using a Bluetooth signal.
With this connection, the device — a coin-sized chip called the “Link” — allows for continuous communication and is designed to not only “read” neural activity but “write” signals into the brain.
Musk has said Neuralink could potentially restore eyesight and motor function for disabled patients and offer the ability to control electronic devices mentally.
Neuralink does not currently have any clinical trials available for enrollment but has created a patient registry for those interested in participating in future trials.
To be eligible for the registry, one must live in the United States, be at least 18 years of age and of consenting age in their state, and suffer from any of a number of medical conditions, including quadriplegia, paraplegia, or vision or hearing loss.
As with any new technology, there are considerable health concerns associated with the Link. Reuters reported in March that the FDA rejected a 2022 application from Neuralink to commence human trials, citing “concern” over the device’s lithium battery, a risk of some of the Link’s wiring to “migrate to other areas of the brain,” and safety questions about the removal of the device without damaging brain tissue.
In animal trials conducted between 2017 and 2020, the device has seen mixed results, with some monkey test subjects using their brain to move computer cursors. But more than half reportedly died from brain hemorrhages or other causes.
While some Christian neurologists have raised ethical questions about implanting devices into human brains, Musk has said his inspiration behind the company in the first place was to be a “risk mitigation for digital super-intelligence.”
“The reason I created Neuralink long-term as a risk mitigation for digital super-intelligence, in that if we are able to effectively achieve symbiosis with digital intelligence, then … the collective human will is better able to steer things in the direction that we’d like, or even with benign AI, at least go along for the ride,” he told The Babylon Bee in a 2021 interview.
“We’re already at this point partially a cyborg … in that our phones and computers and applications are a digital extension of ourselves at this point.”
Among other goals, Musk said he’s confident Neuralink will ultimately allow paraplegic or even tetraplegic to operate a phone “faster than someone who has … working hands.”
Dr. Travis Losey, the vice-chair of the department of neurology and co-director of the Comprehensive Epilepsy Center at Loma Linda University in southern California, said in a 2021 interview with The Christian Post that when it comes to the use of brain interface technology, the purpose should be to heal something that was harmed by disease or a disorder.
“The core ethical issue with the brain-computer interface is similar to issues with medication,” he offered. “I think it’s only ethical to use medications when they are being used to restore function that has been lost or affected by a disease. The same principles would apply to brain-computer interfaces.”
The doctor said there is no higher calling for a Christian than to help people affected by disease. He said believers should enter the field to ensure these technologies are used appropriately.
The facade of “safety” around hormonal birth control continues to crumble: Researchers at Oxford Population Health’s Cancer Epidemiology Unit have recently shown that progestin-only hormonal contraceptives, long billed as the “safest” birth control option because of their lack of estrogen, definitively raises one’s risk of breast cancer, similarly to combined hormonal contraceptives (which contain both synthetic estrogen and progestin).
Furthermore, the Oxford researchers found that breast cancer risk, while it declines after discontinuation of hormonal birth control, still remains elevated for ever-users of hormonal birth control (when compared to never-users). Of course, the Food and Drug Administration (FDA) still won’t cop to increased risks for breast cancer for ever-users of birth control — just for current users — and they are also currently evaluating whether to make a progestin-only pill the first-ever over-the-counter birth control pill in the United States.
Unsurprisingly, in another instance of “nothing to see here, folks,” headlines abounded with the results of the Oxford study for a few weeks, carefully emphasizing the “slight” or “small” increase in breast cancer risk. And the experts, of course, were quick to chime in with all the benefits of hormonal contraception, insisting women shouldn’t see this as a reason to go flushing their pills.
So listen, I talk to women about this every single day. You have to talk about risk vs benefit. It is clear that hormonal contraception lowers the risk of ovarian and uterine cancer, but it increases the risk of clotting. When you put that head to head, it’s about individualizing that risk-benefit and option-risk for the woman. If you talk to any OB/GYN, they will say, we have a line, ‘pregnancy is much higher risk than any associated risk with birth control pills or hormonal contraception.’ So you have to have that conversation based on you and your health-care provider.
While I agree that health-care decisions should be made between a woman and her doctor, is it really true, with everything we know about the risks and side effects of birth control (and we know an awful lot), that it’s really that much “safer” than a nine-month pregnancy? Women, after all, tend to be on birth control for years — perhaps even decades — at a time. And the oft-touted benefits of hormonal birth control reducing ovarian and uterine cancers? Well, Dr. Ashton might be surprised to learn that pregnancy has those, too.
It’s also worth mentioning that while ovarian and uterine cancers can undoubtedly be devastating diseases, the average woman’s baseline risk for breast cancer is far greater than her risk for ovarian or uterine cancer; in fact, breast cancer is now the world’s most commonly diagnosed cancer. In other words, elevating the average woman’s risk of breast cancer even a little bit should be a serious consideration for doctors and health-care institutions indeed. In fact, one might argue they have a moral imperative to help women lower their risks for breast cancer.
Unfortunately, despite increasing, high-quality evidence of the harms of birth control (of which breast cancer is only one among a lengthy list of risks), health-care organizations such as the FDA are loath to give women true informed consent about these drugs. In 2019, the Contraceptive Study Group (CSG) submitted a Citizen Petition to the FDA requesting they add a black box warning to hormonal contraceptives given the mounting evidence for breast cancer risks for ever-users of these drugs (evidence the Oxford study has yet again corroborated).
Yet in a partial response to the CSG’s petition, published a full three years later in 2022, the FDA refused to supply women with this warning. One wonders what leg they have to stand upon now, and if they’ll continue to ignore these significant risks to women — which can be entirely avoided through the use of highly effective, drug- and side-effect-free measures for family planning known as fertility awareness-based methods.
With the publication of the Oxford study, the FDA has once again proven itself at odds with the best scientific evidence on this matter, which even the National Cancer Institute acknowledges. Again, this is largely because of the “benefit” of preventing pregnancy, which evidently trumps all other considerations — even ones that could take the lives of women.
Grace Emily Stark is a freelance writer with published work in multiple outlets, and she is the Editor of Natural Womanhood. Grace is also a current Ramsey Institute Fellow at the Center for Bioethics & Culture, and a former Novak Alumni Fund Journalism fellowship recipient. Follow her writing at GraceEmilyStark.com.
In his 67-page straight-talking opinion, Judge Matthew Kacsmaryk stuck to the facts — something Americans desperately need to hear after decades of euphemistic discussions about abortion.
“Unborn humans.” “Eugenics.” “Head, hands, and legs, with defined fingers and toes.” “Shame, regret, anxiety, depression, drug abuse, and suicidal thoughts.”
Federal Judge Matthew Kacsmaryk’s Friday decision freezing the FDA’s approval of the abortion-pill combination, mifepristone and misoprostol, included these phrases and more. And while the left is already attacking Kacsmaryk’s 67-page straight-talking opinion in Alliance for Hippocratic Medicine v. FDA by framing it as filled with anti-abortionrhetoric, the Trump appointee stuck to the facts — something Americans desperately need to hear after decades of euphemistic discussions about abortion.
After a brief introduction in which Kacsmaryk highlighted the FDA’s two decades of stonewalling that delayed a legal challenge to the 2000 approval of the abortion drugs, the court opened with the basic facts. The plaintiffs — doctors and medical associations that provide health care to pregnant and post-abortive women and girls — sued the FDA, challenging several administrative actions related to the approval of the chemical abortion drugs.
‘Unborn Humans’
The court then explained the drugs and their functioning: “Mifepristone — also known as RU-486 or Mifeprex — is a synthetic steroid that blocks the hormone progesterone, halts nutrition, and ultimately starves the unborn human until death.” But “because mifepristone alone will not always complete the abortion,” the court continued, “the FDA mandates a two-step drug regimen: mifepristone to kill the unborn human, followed by misoprostol to induce cramping and contractions to expel the unborn human from the mother’s womb.”
Calling an unborn human an “unborn human” immediately triggered abortion activists, but as Kacsmaryk explained in a footnote, such terminology is scientifically correct, whereas the lawyers and courts “often use the word ‘fetus’ to inaccurately identify unborn humans in unscientific ways.”
“The word ‘fetus,’” Kacsmaryk explained, “refers to a specific gestational stage of development, as opposed to the zygote, blastocyst, or embryo stages.” And because the FDA’s approval of the abortion drugs applies at multiple “gestational stages,” the word “fetus” would be inaccurate.
It is understandable that abortion activists want to hide the humanity of unborn humans, but that doesn’t make the science less real: It just means girls and women who have bought the “clump of cells” narrative will suffer when faced with the truth, which chemical “at home abortions” force.
“The mother seeing the aborted human ‘appears to be a difficult aspect of the medical termination process which can be distressing, bring home the reality of the event and may influence later emotional adaptation,’” the court wrote, based on the record evidence. “For example, one woman was surprised and saddened to see that her aborted baby ‘had a head, hands, and legs’ with ‘[d]efined fingers and toes.’”
Another woman alleged that “she did not receive an ultrasound or any other physical examination before receiving chemical abortion drugs from Planned Parenthood.” According to the record, “The abortionist misdated the baby’s gestational age as six weeks, resulting in the at-home delivery of a ‘lifeless, fully formed baby in the toilet,’ later determined to be around 30-36 weeks old.”
Harm to Women
Beyond exposing the reality that abortion kills an unborn human, Kacsmaryk’s opinion also refuted the “popular belief and talking points” that using the abortion pill is “as easy as taking Advil.” Here, the federal judge detailed the factual evidence. Among other things, “bleeding from a chemical abortion, unlike surgical abortion, can last up to several weeks,” and by being done at home, “without physician oversight,” it can lead “to undetected ectopic pregnancies, failure of rH factor incompatibility detection, and misdiagnosis of gestational age — all leading to severe or even fatal consequences.”
The opinion also countered the claim that side effects are rare by highlighting evidence that “over sixty percent of women and girls’ emergency room visits after chemical abortions are miscoded as ‘miscarriages’ rather than adverse effects to mifepristone.”
The evidence also shows emotional and psychological injury, Kacsmaryk stressed, with 77 percent of women who underwent a chemical abortion reporting “a negative change” after the at-home abortion, and 38 percent of women reporting issues “with anxiety, depression, drug abuse, and suicidal thoughts because of the chemical abortion.”
While the abortion industry prefers to cite its own evidence, as Kacsmaryk noted, those studies are flawed both because of the miscoding of chemical abortions as miscarriages and because the FDA stopped requiring the reporting of non-fatal adverse reactions.
Eugenic Roots
The left also didn’t like Kacsmaryk exposing the eugenic beliefs of the Population Council, which had sought FDA approval for the abortion drugs. John D. Rockefeller founded the Population Council in 1952, “after he convened a conference with ‘population activists’ such as Planned Parenthood’s director and several well-known eugenicists,” the court wrote. Attendees of that conference discussed “the problem of ‘quality,’” and concluded that “[m]odern civilization had reduced the operation of natural selection by saving more ‘weak’ lives and enabling them to reproduce,” thereby resulting in “a downward trend in … genetic quality.”
“[m]odern civilization had reduced the operation of natural selection by saving more ‘weak’ lives and enabling them to reproduce,” thereby resulting in “a downward trend in … genetic quality.” …….. “Natural Selection”????? Can you say, “disciples of Margarete Sanger”?
Many Americans remain oblivious to the historical backdrop eugenics played to the abortion movement, and activist groups prefer they remain in the dark. The sunlight Kacsmaryk shined upon that truth infuriates them.
Political Pressure
Judge Kacsmaryk also exposed the political pressure placed on the FDA to approve the abortion drug — something Americans are likely to appreciate more today in the aftermath of the FDA’s hasty approval of the Covid mRNA shots.
In the case of the abortion pill, the FDA took the unprecedented step of arranging a meeting between the French pharmaceutical company that owned the patent rights and the eventual drug sponsor, the Population Council. “The purpose of the FDA-organized meeting was ‘to facilitate an agreement between those parties to work together to test [mifepristone] and file a new drug application.’”
Evidence further shows the Department of Health and Human Services “initiated” another meeting to determine how the Clinton administration “might facilitate successful completion of the negotiations” between the French firm and the Population Council to ensure the group secure patent rights and eventual FDA approval.” In fact, Clinton’s HHS secretary “believed American pressure on the French firm was necessary.”
Then after the Population Council submitted a new drug application, the FDA proposed detailed restrictions to address safety concerns, including that the drug be administered by doctors “trained and authorized by law” to perform surgical abortions; trained in administering mifepristone and treating adverse events; and able to provide treatment at a medical facility that had the equipment necessary to perform surgical abortions, resuscitation procedures, and blood transfusion, within one hour’s drive. The FDA’s restrictions were leaked to the press, prompting a political firestorm.
So Much for Safety
The FDA later abandoned the above safety mandates and approved the drug for use to kill unborn humans aged seven-weeks gestation or younger. The FDA further required three “in-person office visits: the first to administer mifepristone, the second to administer misoprostol, and the third to assess any complications and ensure there were no fetal remains in the womb.” All adverse events were also required to be reported.
In 2002, the FDA removed even more of the safety restrictions, increasing the maximum gestational age from seven-weeks gestation to 10-weeks gestation, reducing the number of office visits from three to one, increasing the drug dosage, allowing non-doctors to prescribe and administer chemical abortions, and eliminating the requirement for non-fatal adverse reactions to be reported. Then in 2019, the FDA approved a generic version of the abortion pills, and on April 12, 2021, the FDA announced it would allow abortion pills to be dispensed through the mail.
“Whether FDA abandoned its proposed restrictions because of political pressure or not,” the court wrote, “one thing is clear: the lack of restrictions resulted in many deaths and many more severe or threatening adverse reactions.” But “due to FDA’s lax reporting requirements, the exact number is not ascertainable,” Kacsmaryk stressed.
Straight Facts
But it was not on politics that Kacsmaryk based his decision to freeze the FDA’s approval of the abortion pill. Rather, in his methodical opinion, the federal judge explained that the FDA lacked the authority to accelerate approval of the drug under what is called “Subpart H” of the FDA. That subpart only allows for accelerated approval of drugs that treat “serious or life-threatening illnesses” — something pregnancy is not.
Kacsmaryk also concluded the evidence the FDA supposedly relied upon to approve the abortion drugs failed to support the conclusion that they were “safe and effective under particular conditions of use.” And finally, Kacsmaryk held the FDA’s approval of mail distribution violated the 1873 Comstock Act, which makes it illegal to use the mail to deliver any “article or thing designed, adapted, or intended for producing abortion.”
The Biden administration has already filed a notice of appeal with the Fifth Circuit Court of Appeals, and in issuing his opinion in Alliance for Hippocratic Medicine v. FDA, Kacsmaryk entered a temporary stay, which he or the court of appeals will likely make permanent pending resolution of the case. Thus, abortion pills will remain available for now.
How the Fifth Circuit and eventually the Supreme Court will rule remains to be seen, but what is clear now is the abortion-loving left is desperate to keep the truth about abortion from the public and is furious that Kacsmaryk dared to expose the reality: Abortion kills unborn humans.
Margot Cleveland is The Federalist’s senior legal correspondent. She is also a contributor to National Review Online, the Washington Examiner, Aleteia, and Townhall.com, and has been published in the Wall Street Journal and USA Today. Cleveland is a lawyer and a graduate of the Notre Dame Law School, where she earned the Hoynes Prize—the law school’s highest honor. She later served for nearly 25 years as a permanent law clerk for a federal appellate judge on the Seventh Circuit Court of Appeals. Cleveland is a former full-time university faculty member and now teaches as an adjunct from time to time. As a stay-at-home homeschooling mom of a young son with cystic fibrosis, Cleveland frequently writes on cultural issues related to parenting and special-needs children. Cleveland is on Twitter at @ProfMJCleveland. The views expressed here are those of Cleveland in her private capacity.
Suppose a troubled teen girl “identifies” as a boy and wants to change her body to match it. Most people balk at the thought of pumping her with testosterone or cutting off her healthy breasts. But many of these same people think using puberty blockers isn’t so bad for even younger kids. In fact, activist groups such as the American Academy of Pediatrics suggest drugs like Lupron can “pause” puberty without harm.
Even some conservative lawmakers, such as Georgia state Sen. Carden Summers, have bought this claim. As a result, the bill he sponsored, just signed into law by Gov. Brian Kemp, partially restricts “gender-affirming” hormones and surgeries for minors but says nothing about puberty blockers.
Is it really safe to give these drugs to kids? Mounting evidence says “no.” And even some on the left are starting to sound the alarm.
Last month, a stunning report in the British Medical Journal, written by a former editor of Ms. Magazine, argued that only a contrived medical consensus, not scientific evidence, props up wrongly named “gender-affirming care” for minors. That’s the protocol that starts with social transition, moves on to puberty blockers, then wrong-sex hormones, and finally surgery. The article pointed to disagreement within the medical community about how to best treat kids with gender dysphoria. Indeed, the publication of such an article, in a major medical journal, is itself evidence of such disagreement.
Two weeks earlier, Jamie Reed, a self-identified “queer socialist” married to a “transman,” blew the whistle on the work of the Washington University Transgender Center at St. Louis Children’s Hospital. She confirmed what critics have long been saying: These treatments are uncontrolled experiments with children as subjects.
“These treatments are uncontrolled experiments with children as subjects. “
Lupron
Consider Lupron. First approved by the FDA to treat prostate cancer, doctors later used the drug to chemically castrate sex offenders and stop early-onset puberty.
Today, it’s the primary “off-label” drug used to “block” puberty. Lupron stops the body’s normal hormonal process, including the development of ovaries and testes, by “blocking” the brain’s ability to communicate with the pituitary gland. The pituitary controls the release of hormones. Without it, the sex hormones can’t direct puberty as they otherwise would.
Lupron’s side effects are so severe that doctors tend not to prescribe it for even mild (non-metastatic) cases of prostate cancer. Would you be shocked to learn it might not be great for young girls, either? In fact, after taking the drug, girls may develop osteoporosis and osteopenia, problems that mostly afflict older women. Many doctors found that Lupron decreased minors’ bone density so much that they could no longer recommend it.
Not Reversible
Some gender-activist doctors will admit their guidance is not based on long-term studies. Rather, they claim it’s based on expert consensus.
But that consensus is highly stage-managed. Because of the known dangers and lack of long-term data, the Finnish, French, and Swedish governments have either banned or limited Lupron’s use for minors. Similarly, the British National Health Service now urges caution, and argues most gender-confused minors are going through a “transient phase.”
The report in the British Medical Journal shows this regimen for minors is not based on sound science. The Endocrine Society found that little evidence supports its own guidance regarding Lupron. The Swedish government confirms Lupron does not help these minors. In fact, it “may lead to a deteriorating of health and quality of life,” and can cause irreversible harm.
When used for minors with gender distress, over 95 percent will move on to cross-sex hormones and never go through natural puberty. Even when puberty blockers are discontinued, their dangers to a child’s development don’t disappear. After all, no one can reverse time. It’s no surprise New Zealand’s ministry of health recently scrubbed the words “reversible” from its online discussion of puberty blockers.
Jamie Reed’s firsthand testimony is damning. Patients in Reed’s clinic could access hormone blockers after only one meeting with a therapist. Some of these minors had severe mental illnesses that went untreated. Instead, they were fast-tracked with transgender drugs toward transition surgeries.
States Start to Respond
Fortunately, the word is getting out. Some states are now restricting these weapons in the “gender-affirming” arsenal. Since 2022, Alabama, Arkansas, Arizona, Mississippi, South Dakota, Tennessee, Utah, and Iowa have passed legislation to restrict Lupron as a puberty blocker. (Alabama and Arkansas’ bans are on hold in federal district court.) Several more states will likely do so in the coming weeks.
Florida followed another path to ban this use of Lupron. The state’s medical boards reviewed the literature and found these transition procedures lacked a solid scientific basis. The legislature is now working to secure their boards’ judgment in law.
Other states should follow Florida’s lead and pass health policies and laws that follow scientific evidence, not the activists’ spin. Until this happens, troubled children will continue to be sacrificed on the altar of toxic ideology.
Samuel Silvestro is a member of The Heritage Foundation’s Young Leadership Program. Jay W. Richards is the director of Heritage’s DeVos Center for Life, Religion, and Family.
Typically, a lack of efficacy and a cataclysmic level of hundreds of different side effects would be reason to take a therapeutic off the market. But in the post-Nuremberg Code era we find ourselves in, such outcomes serve as a resume enhancer for the product. The FDA is planning a blitz of increased approvals of the shots on the youngest of Americans, yet not a single national Republican has stood up and said “No.” Only one governor, Ron DeSantis, has recommended against their use in children. Which will be the first state to block implementation of the FDA’s new therapeutic jihad on behalf of Big Pharma?
The FDA’s Vaccines and Related Biological Products Advisory Committee (VRBPAC) has an ambitious schedule for this coming June. Here are its upcoming meetings.
June 7: Approval of Novavax first time for those over 18.
June 8: Approval of Moderna in teenagers.
June 21: Approval of Moderna in kids under 6.
June 22: Approval of Pfizer in kids under 5.
June 28: Exploring new shots for new variants.
Isn’t it interesting how they are meeting about the need for new shots for the current variants after already likely approving old shots on babies who don’t need the shots and for a variant that hasn’t existed for over a year?
Here we have many European countries banning the Moderna shot on those under 30 because of myocarditis, yet our government will likely expand its use to babies at a whopping dose of 25 micrograms! We now have over 1.2 million adverse events reported to VAERS, and CDC researchers admitted in a JAMA paper that the myocarditis numbers – just shy of 40,000 – are “likely” underreported. Also, we now know that Pfizer and the FDA knew about 1,223 deaths shortly after release. As for Moderna, we don’t have a single court-released document from the company yet, so who knows what they are hiding?
It would be one thing to approve something that worked amazingly for COVID despite terrible side effects. But the shot is a complete bust.
The expectation of negative efficacy from these shots has become so widely accepted that now the only question is who is the next famous politician or celebrity to get COVID multiple times after having gotten three or four shots. Take a look at this chart from the Walgreens COVID-19 index of all its testing this past week broken down by vaccination status:
Have you ever seen a vaccine of which the more doses you get, the more likely you are to test positive? Notice how the unvaccinated account for a lesser share of cases than either their share of the population or of Walgreens-administered COVID tests. The results are based on 81,818 tests administered nationwide in Walgreens stores from May 2 through May 8.
So now they want to take vaccines with such counterproductive outcomes and foist them upon children? Remember, the FDA has already demanded the manufacturers produce a study on subclinical myocarditis. In its Pharmacovigilance Plan Review Addendum for Comirnaty, the agency cited one study at the time of Pfizer’s approval noting that subclinical myocarditis might be 60 times as prevalent as clinical myocarditis. That would bring down the 1 in 1,000 rate among young males to as low as 1 in 17 for subclinical ticking time bombs!
Let’s not forget that in all the children’s trials, there were zero deaths and hospitalizations in the placebo groups. So, what exactly were we trying to protect against – even before we knew the shots weren’t effective and possibly negatively effective? Cold or flu-like symptoms? Well, here is the data of side effects from Moderna’s 5-11 trial:
“The most frequently reported adverse reactions were pain at the injection site (92%), fatigue (70%), headache (64.7%), myalgia (61.5%), arthralgia (46.4%), chills (45.4%), nausea/vomiting (23%), axillary swelling/tenderness (19.8%), fever (15.5%), injection site swelling (14.7%) and redness (10%).”
So even before we get to more serious side effects like heart inflammation, we have a massive percentage of children getting flu-like symptoms from the shots, which is what they would get anyway from the virus. How can this pass the threshold of any principle laid out in the Nuremberg Code or the Helsinki Declaration?
It’s gotten so bad that Pfizer and Moderna can no longer rely upon dubious trials showing a 90% reduction in COVID. Especially for young children, even for mild infection, they couldn’t even manipulate any data showing any degree of efficacy, so they had to rely on an arbitrary measure of antibody titers rather than clinical outcomes. In shocking statement before the House Select Subcommittee on the Coronavirus Crisis, Peter Marks, director of the FDA’s Center for Biologics Evaluation and Research, conceded they would approve the shots on young children even if the manufacturer’s own dubious data shows less than 50% efficacy (and even that is only for minor illness).
“If these vaccines seem to be mirroring efficacy in adults and just seem to be less effective against Omicron like they are for adults, we will probably still authorize” because they nonetheless reduce the risk of severe disease in the mildest COVID variant, Marks revealed during the May 9 briefing.
Just keep in mind that, according to the CDC, 74.2% of kids 0-11 already got natural immunity from prior infection. So not only will they fail to test kids for antibodies before injecting them, but even the remaining quarter who might be COVID-naive, they are trading risk of death and severe side effects (and pervasive mild side effects) for a possible tiny degree of very short-term efficacy against sniffles, but a long-term negative efficacy against those sniffles. A preprint study by the NY State Department of Health in February showed that the Pfizer shot was just 12% effective against the first Omicron variant for 5- to 11-year-olds, but drops to -41% after just 42 days!
How can any of these shots be administered until we understand why so many data points seem to show intensifying negative efficacy with time? It’s like investing in a stock that first goes up for a few weeks, but then you erase all the gains within a few days and then gradually lose all your principal investment. Every Republican claims to be pro-life, but distributing these shots to young children is not pro-life, even if they are not quite mandated. Would they sit idly by if the federal government distributed abortifacients throughout their states?
They are not even trying to convince us any more. They are now using brute force to coerce us into COVID fascism, including forced injections, so they have no need to even hide their false information.
In Pfizer’s FDA briefing document prepared for the Oct. 25 meeting was an admission that even according to the company’s own unverified and misleading math, there is a scenario where there would be more hospitalizations among children for myocarditis — just one side effect — than from COVID. “Under Scenario 3 (lowest incidence), the model predicts more excess hospitalizations due to vaccine-related myocarditis/pericarditis compared to prevented hospitalizations due to COVID-19 in males and in both sexes combined,” states Pfizer in page 33 of the document.
How in the world could there be any universe where we would approve a shot, much less promote and force it in many settings, when there is a possibility of greater harm than benefit, when the harm is man-made and the virus is left to chance? They know quite well that this approval will eventually lead to soft and hard mandates, which have already begun in California schools.
The document concludes by expressing the same callous attitude toward those raising concerns as toward all their interventions from day one. “However, in consideration of the different clinical implications of hospitalization for COVID-19 versus hospitalization for vaccine-associated myocarditis/pericarditis, and benefits related to prevention of non-hospitalized cases of COVID-19 with significant morbidity, the overall benefits of the vaccine may still outweigh the risks under this lowest incidence scenario.” In other words, sure, we have no clue what’s going to happen, but it’s always better to err on the side of shoving this on children who have a 99.9% recovery rate.
Moreover, there are a couple of obvious factors that demonstrate clearly, by their own admission, the shots pose more risk than benefit:
Already in March, 42% of children 5-17 have had the virus, according to the CDC, and that number is likely much higher following the prolific spread of the Delta variant. So the benefit in terms of lives saved is much less than they predict, because the majority of children likely already have protection even from mild illness. We are not beginning with a clean slate with 100% of children vulnerable to getting the virus. Plus, studies have shown among adults that those who already had the virus not only don’t need a vaccine, but these shots pose a greater risk to them than to those without prior infection.
Even the infinitesimal risk of serious illness among young children is clearly limited to a very defined pool of very sick and severely obese children. It would be one thing to just make it available for those children. But if you isolate healthy children, it’s quite evident that so many more lives would be lost than saved because healthy children essentially do not get seriously ill from this virus.
COVID hospitalizations among children are grossly exaggerated in the data and conflated with those admitted for other ailments who just had COVID incidentally. A study published in the Journal of American Academy of Pediatrics found, “Nearly one-half of the infected children had coinfection with other common respiratory pathogens.” Scientists from University College London and the Universities of York, Bristol, and Liverpool studied the data from all pediatric COVID-19 infections in the U.K. and found that 61% of the reported pediatric COVID deaths were overstated.
This analysis still assumes that the vaccines are over 90% effective. In reality, Sweden’s extremely large study has shown that the efficacy wears off to zero after seven months, and the U.K data demonstrate that thereafter the vaccinated are more likely to get COVID than unvaccinated people. Thus, if the entire benefit of injecting children, as suggested by Pfizer, is to prevent mild non-hospitalized cases, the vaccines actually contribute to the risk incurred, not the benefits reaped from the shots.
This analysis ignores the fact that there are numerous other treatment options for children and adults alike that will reduce chances of death without causing side effects like myocarditis. We need not be faced with the false dichotomy between poisonous shots and not treating the virus. Why are these shots getting approval for children’s use before the monoclonal antibodies, which are much safer and have been shown to work even pre-emptively up to eight months later?
Are we really going to trust Pfizer’s numbers? In reality, independent studies have found the risk of myocarditis to be much worse. A preprint from University of California Davis found that “for boys 12-15 without medical comorbidities receiving their second mRNA vaccination dose, the rate of CAE [cardiac adverse event ] is 3.7 to 6.1 times higher than their 120-day COVID-19 hospitalization risk as of August 21, 2021.” A recent study of the Danish population published in the Pediatric Infectious Disease Journal found that “the incidence of myopericarditis after COVID-19 vaccination among males appears higher than reports from the United States.” Have you ever wondered why it always seems that the negative information on the vaccines is downplayed and the supposed positive benefits are exaggerated in the U.S. more than elsewhere? Clearly, the signals regarding cardiovascular side effects are greater than U.S. authorities are willing to admit. In September, the U.K. Telegraph reported, “Data from Public Health England (PHE) shows that during that period there were 2,103 extra death registrations with ischemic heart disease, 1,552 with heart failure, as well as an extra 760 deaths with cerebrovascular diseases such as stroke and aneurysm and 3,915 with other circulatory diseases.”
The question everyone should be asking is, “What is the Number Needed to Vaccinate (NNTV) to prevent a single COVID-19 fatality in this age group, and how many people will we kill, maim, and weaken their immune systems on the way to achieving that number?” Dr. Toby Rogers, an economist and statistician, laid out the numbers in simple arithmetic last week. He concludes that if you give Pfizer 80% effectiveness against the 57 reported fatalities over this six-month period, it would work out to saving 45 lives after vaccinating 28 million children. So, the NNTV to prevent a single COVID death would be 630,775 (28,384,878 / 45), but because it’s a two-dose regimen, you would need 1,261,550 total injections.
Now what about the risk? If you take the 128 reported vaccine deaths among those ages 12-24 as a baseline, then utilize Kirsch, Rose, and Crawford’s estimate that VAERS undercounts fatal reactions by a factor of 41, that would amount to 5,248 fatal side effects during the same period of time. Thus, in order to save 45 children, we’d kill 5,248 — for a ratio of one kid saved for 117 killed. And again, this analysis doesn’t account for the fact that for healthy children, there are essentially zero COVID deaths, more than half the children likely already had COVID, there are other treatments available, and on the risk side, we don’t know if there are long-term side effects that will create excess deaths well beyond the shot’s six-month window of efficacy.
Additionally, we don’t even know if those getting the shot now will enjoy anywhere near this degree of efficacy given that the virus is rapidly changing. What we do know, however, from the adult vaccinations, is that adults are more vulnerable to the virus for the first month, then again as the vaccine wanes after six months. Plus, Pfizer’s trial shows that more than half the children experienced cold or flu-like symptoms from the shots. So they admit that there were no cases of serious illness in the control group and are thus using the shot to merely prevent a flu, yet it will likely give them flu-like symptoms up front and make it more likely they will get the virus after six months.
Indeed, there has never been such a lopsided risk-benefit ratio to any medical device approved by our government, even on a limited basis, much less used to bribe and shame children into injecting. As Dr. Eric Rubin, member of the FDA’s advisory committee on vaccines and editor of the New England Journal of Medicine, said during the Oct. 26 meeting: “We’re never going to learn about how safe the vaccine is unless we start giving it, and that’s just the way it goes.”
Editor’s note: This article has been corrected to note that Dr. Rubin is a member of the FDA’s advisory committee on vaccines, rather than the CDC’s Advisory Committee on Immunization Practices (ACIP).
A company mentioned as a fetal tissue supplier in recent Planned Parenthood sting videos reportedly does business with two federal health agencies. According to a report in Politico, Advanced Bioscience Resources, a contracting research company, has made over $300,000 in transactions with the National Institutes of Health and Food and Drug Administration. Both agencies reportedly had contracts with the firm since 2009, and have paid money for materials in order to conduct various types of research, including HIV and eye disease studies.
Politico reports it’s unclear if the firm got any tissue from abortions at Planned Parenthood, though the company was mentioned in one of the recent videos released by an anti-abortion group. Those videos show Planned Parenthood officials discussing fetal tissue harvesting.
Officials reportedly said NIH has paid the ABR firm $257,000 since 2009 and $53,000 last year alone. The officials, however, didn’t explain how much of the money went toward fetal tissue and how much went to other supplies. The report added that some tissue came from 17- to 22-week-old fetuses. Multiple anti-abortion organizations want to prohibit most abortions after 20 weeks.
The FDA also paid the firm $73,000 in the same amount of time. Officials told Politico that much of that money was for certain liver and thymus tissue in order to test drug therapies.
The firm did not return Politico’s requests for comments.
American Family Association
American Family Association (AFA), a non-profit 501(c)(3) organization, was founded in 1977 by Donald E. Wildmon, who was the pastor of First United Methodist Church in Southaven, Mississippi, at the time. Since 1977, AFA has been on the frontlines of Ame
NEWSMAX
News, Opinion, Interviews, Research and discussion
Opinion
American Family Association
American Family Association (AFA), a non-profit 501(c)(3) organization, was founded in 1977 by Donald E. Wildmon, who was the pastor of First United Methodist Church in Southaven, Mississippi, at the time. Since 1977, AFA has been on the frontlines of Ame
American Family Association
American Family Association (AFA), a non-profit 501(c)(3) organization, was founded in 1977 by Donald E. Wildmon, who was the pastor of First United Methodist Church in Southaven, Mississippi, at the time. Since 1977, AFA has been on the frontlines of Ame
You Version
Bible Translations, Devotional Tools and Plans, BLOG, free mobile application; notes and more
Political
American Family Association
American Family Association (AFA), a non-profit 501(c)(3) organization, was founded in 1977 by Donald E. Wildmon, who was the pastor of First United Methodist Church in Southaven, Mississippi, at the time. Since 1977, AFA has been on the frontlines of Ame
NEWSMAX
News, Opinion, Interviews, Research and discussion
Spiritual
American Family Association
American Family Association (AFA), a non-profit 501(c)(3) organization, was founded in 1977 by Donald E. Wildmon, who was the pastor of First United Methodist Church in Southaven, Mississippi, at the time. Since 1977, AFA has been on the frontlines of Ame
Bible Gateway
The Bible Gateway is a tool for reading and researching scripture online — all in the language or translation of your choice! It provides advanced searching capabilities, which allow readers to find and compare particular passages in scripture based on























You must be logged in to post a comment.