Protesters march Aug. 3 in London in the wake of Dr. Hilary Cass’ warning about the harms of so-called gender-affirming care. A newly revealed email shows a U.S. health official supports “puberty blockers” while admitting they increase the risk of suicide. (Matthew Chattle/Future Publishing/Getty Images)
FIRST ON THE DAILY SIGNAL—Former officials in the U.S. Department of Health and Human Services and the Food and Drug Administration condemned what they described as the FDA’s duplicity in allowing off-label use of so-called puberty blockers while loudly condemning the use of far safer drugs to treat COVID-19.
“During the Trump administration, the media falsely accused us daily of ‘politicizing America’s public health agencies.’ Yet the same media is now silent on [Vice President Kamala] Harris and [President Joe] Biden’s FDA’s anti-science, purely political insanity,” Brian Harrison, former chief of staff at HHS and now a member of the Texas House of Representatives, told The Daily Signal in a written statement.
“We’ve now learned that the same FDA that banned mothers from importing safe formula for starving babies and kept safe COVID treatments from patients was apparently pushing dangerous puberty blockers for kids,” Harrison added.
In the Jan. 25, 2022, email, Shannon Sullivan, clinical team leader at the FDA’s Division of General Endocrinology, noted that the agency’s Division of Metabolism and Endocrinology Products performed a “safety review of the GnRH agonist class in pediatric patients in 2016/2017.”
GnRH stands for “Gonadatropin-releasing hormone.” GnRH agonists prevent the natural release of testosterone and estrogen that initiate puberty.
“Our review focused on suicidal ideation/depression, seizures, and bone health,” Sullivan wrote in the 2022 email. Although most of the minors in the study suffered from central precocious puberty (in which puberty starts too early), she said, “a handful were transgender kids using the drugs off-label.”
“We found no effect on bone (after factoring in catch-up growth), including no increase in fracture risk,” she noted. “We did find increased risk of depression and suicidality, as well as increased seizure risk and we issued [safety-related labeling changes].”
Yet, as The Daily Signal reported, Sullivan went on to recommend approving GnRH agonists for minors.
The FDA’s Division of Urology, Obstetrics, and Gynecology, she wrote, “has done a patient listening session with trans kids and separately with trans adults, which I participated in, and there is definitely a need for these drugs to be approved for gender transition, as they are typically not covered by insurance and are expensive out of pocket.”
Sullivan also said that “no company has come in” to provide “GnRH agonists in the transgender population” yet. However, she added, “it was my understanding” that the FDA division “would take these applications if and when they do come in.”
Screenshot
Transgender activists claim that minors who identify with the gender opposite their biological sex need experimental medical alterations such as GnRH agonists either to prevent puberty or to force their bodies to resemble the bodies of the opposite sex. Activists mask the nature of these interventions with the term “gender-affirming care” and insist that without these interventions, kids will commit suicide.
Roger Severino, former director of the Office of Civil Rights at HHS and now vice president of domestic policy at The Heritage Foundation, emphasized the contradiction between the rhetoric supporting “gender-affirming care” and the findings noted by the FDA’s Sullivan.
“HHS still claims puberty blockers for 12-year-olds are fully ‘reversible,’ seemingly oblivious to the fact that suicide is as irreversible as it gets,” Severino quipped.
FDA’s Duplicity on COVID-19, ‘Puberty Blockers’
David Gortler, a Yale University-trained pharmacologist who previously was a senior adviser to the FDA commissioner on policy and drug safety, raised the alarm about GnRH agonists for minors. Gortler told The Daily Signal that the Food and Drug Administration is being “duplicitous” in how it uses its Adverse Event Reporting System (AERS), a database of reactions to certain drugs that users report to the FDA.
The FDA relied heavily on the reporting system’s data to declare that hydroxychloroquine was unsafe after finding only a few hundred reports of adverse events, he said, but the agency dismisses a considerably higher number of such reports for GnRH agonists.
“GnRH agonists account for 70,000 adverse reports,” Gortler said. “While these reports still need to be reviewed, it is a remarkable number of adverse events for what should be a niche, otherwise rarely clinically indicated, class of drugs.”
Yet the FDA often dismisses these reports as “not confirmed”; “not establishing causation”; “no definitive proof”; and “not establishing a rate of occurrence.”
Gortler, who has analyzed the data himself, showed that preliminary analysis to The Daily Signal. According to his analysis, AERS reports 70,000 adverse reactions to GnRH agonists, 2,510 of them involving children aged 14 or younger.
Adverse reactions include hallucinations, bone disorders, cardiac arrest, abdominal pain, migraine, mood alterations, a clot in the heart, pelvic pain, seizures, abnormal skin odor, blindness, and more. Among patients ages 4 to 13, a total of 21 had thoughts of suicide.
The AERS database includes 30 records noting the death of a patient between the ages of zero and 14 where a “puberty blocker” is the primary suspect drug.
These cases include a 10-year-old who died of a hemorrhagic stroke after taking Lupron, a brand of synthetic hormone, in March 2014; a 5-year-old who died of cancer reported in May 2022; an 8-year-old who died of liver failure after receiving leuprolide acetate, a synthetic drug, in March 2004; and a 14-year-old who “completed suicide” in April 2017.
“Even though this drug is objectively unsafe, they seem to be selectively turning a blind eye to it, seemingly in sync with White House messaging,” Gortler said, referring to FDA officials.
“At the same time,” he added, “the FDA selectively heavily involved itself in the off-label administration of ivermectin and hydroxychloroquine, both of which were relatively much safer than GnRH agonists, based on clinical studies, randomized controlled trials, AERS reports, plus other epidemiological findings.”
Where Do ‘Puberty Blockers’ Come From?
The former FDA adviser also told The Daily Signal that physicians developed GnRH agonists to help treat certain cancers that depend on estrogen or testosterone. Removing estrogen and testosterone from cancer patients to prolong their lives makes sense, Gortler said, because it prevents the progress of an invasive, malignant disease. But giving these drugs to physiologically and genetically healthy kids is a completely different story, he said.
“This drug was tested, designed, and FDA-approved for use in an older, cancer-afflicted population,” Gortler said.
“The human body has around 100 trillion cells,” Gortler noted. “High school biology taught us that in each of those nucleated cells, there are either XX or XY chromosomes denoting a female or male sex, respectively. No drug or medical procedure will ever be able to fight 100 or so trillion cells and trying to do so would be a fool’s errand.”
He compared “puberty blockers” to the outdated, dangerous custom of Chinese foot binding, in which a young girl’s feet would be tightly wrapped to keep them from growing naturally.
“Similarly, GnRH agonists block a normal, healthy development process from occurring,” Gortler said. “Just because it’s not something that isn’t directly and obviously visible doesn’t mean that it’s any less clinically, scientifically, or ethically dangerous.”
The FDA did not respond to The Daily Signal’s request for comment.
The truth about transgenderism is coming out. On Monday, Michael Shellenberger released a multitude of internal files from the World Professional Association for Transgender Health (WPATH) that “prove that the practice of transgender medicine is neither scientific nor medical.” WPATH has been accepted by the political, cultural, and medical establishments as the authority on transgenderism, but what its members say in private is not the narrative they sell to the public.
Instead of the rigorous, careful, evidence-based medicine that champions of “gender-affirming care” claim to practice, the WPATH files show doctors who are making it up as they go along, smashing through guardrails even though they know that the children they are chemically and surgically altering cannot really give informed consent. And people are noticing.
No wonder the transgender ideologues are worried. The public has proven more resistant than they expected, especially regarding radical policies such as putting men in women’s prisons and girls’ locker rooms, let alone sexually mutilating and sterilizing children. And transgender activists and their allies have no response except to repeat their same failed arguments, just louder.
Consider a recent opinion piece in the New England Journal of Medicine by Michael R. Ulrich, a Boston University professor of law and public health who is also affiliated with Ibram X. Kendi’s scandal-plagued Center for Antiracist Research. Ulrich argues that restrictions on transitioning children are part of a broader right-wing culture war restricting and regulating medicine. There is a lot wrong with this assertion, but the fundamental problem is that so-called gender-affirming care is not medicine.
From puberty blockers to hormones to surgeries, transition is never medically necessary. Transitioning does not cure any disease or correct any physical ailment or injury. Rather, the point of medicalized transition is to disrupt and destroy the normal functioning of healthy bodies.
Ulrich tries to assuage concerns over these procedures by comparing them to “Pediatric chemotherapy and radiation,” which also “have lasting effects on growth development and reproductive capabilities.” Well, yes, but cancer kills people, which is why we are willing to accept serious side effects to treat it — and even then, doctors and patients have to balance the risks of the disease against the risks of treatment. In contrast, there is no physical risk from not receiving “gender-affirming care,” whereas, as the WPATH files show, there is significant, potentially lethal, risks from puberty blockers, cross-sex hormones, and transition surgeries.
This is why the argument for transition always comes down to encouraging people, especially children, to take themselves hostage by threatening suicide. The only harm that can come from not transitioning is self-harm. And so, Ulrich deploys the suicide threats early and often, writing that “it is not hyperbole to say that lives are at risk in states pursuing these bans on needed care.” Ulrich offers no real evidence to back this claim up. He simply presumes that the “high rates of suicide, suicide attempts, and suicidal ideation among transgender young people” would be reduced with affirmation and medical transition.
Ulrich cites just one study as “evidence showing the effectiveness of gender-affirming care in reducing depression, anxiety, and suicide attempts.” But, despite hype to the contrary, that study showed no such thing. Rather, as Jesse Singal explained after it was published in 2022, “the kids who took puberty blockers or hormones experienced no statistically significant mental health improvement during the study. The claim that they did improve, which was presented to the public in the study itself, in publicity materials, and on social media (repeatedly) by one of the authors, is false” (emphasis in original).
No Evidence Regarding Suicide
There is no good evidence that transition prevents suicide, especially for children. Those who identify as trans do have an elevated risk of suicide (though this tends to be exaggerated by activists), but this is best explained by trans-identified individuals also having a much higher rate of mental health problems and trauma — and it doesn’t help to add to these underlying issues the lie that they were somehow born in the wrong body.
This extraordinary claim — that some children are born into the wrong bodies, and therefore must be chemically and surgically reshaped into a facsimile of the opposite sex — is medically unsupported. It is ideological and sexual fantasy masquerading as medicine. There is no good evidence to support transitioning children because gender ideology is just that, an ideology masquerading as medicine. The reality of human nature does not change, even though much of the medical establishment, such as the NEJM, was shamefully eager to capitulate to a small number of aggressive activists.
Rein in the Industry
Therefore, it is not only reasonable, but imperative, for legislators to rein in the transgender industry, and especially to stop the “transitioning” of children. Ulrich and other activists can fulminate about right-wing conspiracies, but it is right and just to ban the surgical and chemical mutilation of children. Many states have done so, thereby proving that gender ideology will not inevitably triumph and claim our children for its own.
This does not mean the fight is over. Indeed, we should expect gender ideologues to become more aggressive as their losses pile up. They thought time would be on their side, and that new research would vindicate them. But their time is running out, and the continued lack of evidence for “gender-affirming care” is pushing them to increasingly brazen lies and distortions as they attempt to justify their collapsing position. And they are also becoming more authoritarian in the places and institutions they do control, as they attempt to impose transgender dogma on the rest of us.
Thus, those opposed to gender ideology must not get cocky. Trans activists and their allies will keep fighting to the bitter end, especially those who have staked their reputations, livelihoods, and self-respect on radical gender ideology. Nonetheless, the end can now be envisioned, even if much work remains to achieve it.
Nathanael Blake is a senior contributor to The Federalist and a postdoctoral fellow at the Ethics and Public Policy Center.
The Democrats who run California love “transitioning” kids, including chemically and surgically sterilizing them. But a courageous group of residents is betting California voters are less radical than their politicians and that the tide can turn against gender ideology even on the West Coast.
A proposed ballot initiative by Protect Kids California would put the Golden State’s radical “trans kids” agenda — which has previously been checked only by Gov. Gavin Newsom’s presidential ambition — before the people.
The initiative would enact three policies:
First, it would end the practice of government schools socially transitioning children without telling parents. Schools would be required to inform parents about mental health issues, including gender-identity issues, and to have parental permission before pretending a boy is a girl, or vice versa.
Second, the law would require that sex-specific spaces and sports be based on sex, rather than self-declared “gender identity.” Boys would no longer be allowed to participate in girls’ sports or share the girls’ locker room, showers, and other private spaces.
Finally, the law would prohibit medically transitioning children with chemicals, hormones, and surgeries in an impossible quest to change a child’s sex. Chemically castrating boys and amputating the healthy breasts of troubled adolescent girls would be illegal.
These worthy goals might seem impossible. Even as many other states have enacted such policies, California’s leaders have doubled down on radical gender ideology and transitioning children. But the organizers of the initiative point to polling to argue that California’s voters are on their side on this issue, even if Californians tend to vote for Democrats who are in the grip of gender ideology and the transgender lobby. Erin Friday, one of the leaders of the effort, is a lifelong Democrat, and she is convinced there are many more like her who find the transgender industry’s targeting of children abhorrent.
She may be right. The campaign’s website highlights polling showing that the public is with them, and in an email to me, Friday shared additional polling commissioned by the feminist Women’s Liberation Front showing overwhelming support for the child-protection policies this ballot initiative would enact.
This ballot initiative would protect children from outside California as well. As Friday has explained, California is a sanctuary state for sexual experiments on children. In the name of gender ideology, California now refuses to return runaways to their out-of-state parents, pays for minors to be chemically and surgically castrated, and shields doctors who flee to California after breaking the laws of other states. Winning in California is a victory for everyone.
Thus, California’s Democrat establishment will do everything it can to stop this. The state attorney general has already written a biased and inaccurate summary of the measure (the title line is literally “RESTRICTS RIGHTS OF TRANSGENDER YOUTH”) that by law is included on the petition pages. And additional resistance is sure to follow — for example, petition signatures will be rigorously scrutinized by people who otherwise denounce election-integrity measures as racist.
The debate over the measure will be ugly. Its opponents will undoubtedly resort to suicide threats early and often, declaring that this law will push kids to kill themselves. It won’t, but telling kids to take themselves hostage is the transgender movement’s main weapon. After all, the only harm that can come from not transitioning is self-harm. Furthermore, there is no good evidence that castrating or mutilating kids reduces suicides. And in other contexts, we recognize that constantly threatening suicide is manipulative and abusive.
The ugliness won’t end just because the election does. If this measure gets on the ballot and passes, there will be lawsuits. There will be protests that turn into riots. There will be promises of noncompliance from government officials and employees. But it will all be worth it.
If gender ideology goes down in California, it will fall everywhere. Even the most committed Democrats (and the most craven Republicans — looking at you, Ohio Gov. Mike DeWine) will have to acknowledge that it is a political liability. And the collapse could be swift. Many people went along with radical gender ideology not out of conviction, but because they were afraid of being caught on the wrong side of the latest front in the cultural revolution. They will happily abandon it if their fear is taken away, and defeating transgender radicalism in California will do that.
There is work to do before that happy future is realized. The initiative has yet to qualify for the ballot, let alone pass. California residents can print out the petition, sign it, and mail it in. They can also volunteer. And everyone can donate to help fund the effort. Collecting more than a half-million valid signatures isn’t free, to say nothing of countering the mass of lies the media will tell about it.
But it is worth the attempt. 2023 brought a lot of victories in protecting children in Republican states from transgender insanity, but victory requires going on offense, even — especially — in California.
Nathanael Blake is a senior contributor to The Federalist and a postdoctoral fellow at the Ethics and Public Policy Center.
Up to a third of trans-identified teens put on puberty blockers suffered a significant decline in mental health, according to new analysis of a survey from the United Kingdom.
In August, researchers published an updated review of data from a 2021 study in the U.K. on medRxiv, a preprint service for medical research. The original study conducted by the U.K. National Health Service (NHS) examined 44 children aged 12 to 15 over three years who were prescribed puberty-blocking drugs to treat gender dysphoria. Participants took triptorelin, a prostate cancer medicine used to inhibit the synthesis of estrogen in women and testosterone in men.
According to researchers at the University of Essex, the mental health of between 20 and 34 percent of participants significantly deteriorated while on the puberty-inhibiting drug. Just between 9 and 20 percent reported a reliable improvement. Between 56 and 68 percent witnessed no change in distress.
In other words, less than a fifth of those prescribed puberty-blocking drugs, if that, experienced emotional improvement after taking triptorelin. The findings contradict broad claims that such medical interventions are necessary to save gender-confused children from the perils of suicidal ideation. While the updated analysis from the University of Essex has yet to be peer-reviewed, another long-term study from Sweden found those who underwent transgender surgery were 19 times more likely to die by suicide than the general public.
The national suicide hotline is 1-800-273-8255. More resources are here.
A U.S. study published in 2019 found nearly 60 percent of trans-identified patients in a more than 10,000-patient survey were diagnosed with at least one psychiatric disorder (besides gender dysphoria) to begin with.
In June, the U.K. NHS updated guidelines to prohibit prescriptions for puberty blockers outside of clinical research. The change in protocol follows other European nations similarly pulling back on dangerous premature medical interventions on minors who wish to manipulate their gender.
“In the past few years, European health authorities conducted systematic reviews of evidence for the benefits and risks of puberty blockers and cross-sex hormones,” City Journal reported in February. “The findings from these reviews — that the certainty of benefits is very low — guided the hand of policymakers there to restrict access to hormones.”
On Friday, California Democrat Gov. Gavin Newsom vetoed radical legislation mandating that parents “affirm” a child’s newfound so-called “gender identity.” Parents with kids in California’s Chino Valley Unified School District, however, are still fighting state Democrats for the right to watch over their own children.
In August, California’s far-left Attorney General Rob Bonta launched a legal crusade to terminate the district’s new policy requiring schools to notify parents whenever a child tries to change pronouns or display other symptoms of gender dysphoria.
Tristan Justice is the western correspondent for The Federalist and the author of Social Justice Redux, a conservative newsletter on culture, health, and wellness. He has also written for The Washington Examiner and The Daily Signal. His work has also been featured in Real Clear Politics and Fox News. Tristan graduated from George Washington University where he majored in political science and minored in journalism. Follow him on Twitter at @JusticeTristan or contact him at Tristan@thefederalist.com. Sign up for Tristan’s email newsletter here.
NIH is funding many studies premised upon how little research has been conducted on the long-term health risks of cross-sex hormones. Yet HHS is pushing for more transgender ‘care.’
As the Biden administration pushes the Department of Health and Human Services to make “gender-affirming health care” more widely available, HHS’s own National Institutes of Health is funding multiple studies premised upon how little research has been conducted on the long-term risks of taking cross-sex hormones and whether they improve mental health. The NIH research on transgender issues also emphasizes intersectionality and about half has been on HIV prevention.
The NIH Reporter database, which lists active federally funded research projects, shows 74 with “transgender” in the title, totaling more than $26 million of taxpayers’ money annually. Several NIH-funded studies examine specific health risks of cross-sex hormone treatment — such as associated bone loss and possible increased risk of thrombosis, drug overdose, heart attack, and stroke.
Onlyafew studies evaluate the risk of infertility, even though “the impact of long-term cross-sex hormone therapy on reproductive health is largely unknown,” as one such project states and experts have warned. In contrast, seven studies examine stigma and disparities in health care for transgender people, in response to NIH’s Notice of Special Interest in understanding the role of alleged intersectional stigmas and how they harm health.
Manystudiesaddresshigherincidence of sexually transmitted infections in transgender people, and whether hormone therapy might increase that risk. About half of all NIH-funded research on transgender health, including that which has been completed, relates to HIV prevention among the transgender population, totaling approximately $80 million since 1985.
Transgender males “have some of the highest concentrated HIV epidemics in the world, with a pooled global prevalence of 19% and a 49-fold higher odds ratio of acquiring HIV than non-transgender adults,” according to one project summary. Behavioral factors contribute, another project says, but the role of sex hormones needs further study, since they “are known to modulate the immune response, resulting in changes in host susceptibility to pathogens, vaccine efficacy and drug metabolism.”
Many Ongoing Projects Highlight Lack of Research
While suicide prevention is often cited as a major reason to give dysphoric children puberty blockers and cross-sex hormones, only one of the current studies is focused specifically on suicide risk, although several emphasize the lack of long-term studies of cross-sex hormones administered to children and their relation to mental health.
Medical professionals “say more specific research is needed to determine whether medically transitioning as a minor reduces suicidal thoughts and suicides compared with those who socially transition or wait before starting treatment,” according to Reuters.
One NIH-funded project summary acknowledges that the long-term effect of puberty suppression on mental health needs further study and will evaluate children already taking puberty blockers.
During puberty, hormones change the structure and organization of the brain. Puberty blockers “may also disrupt puberty-signaled neural maturation in ways that can undermine mental health gains over time and impact quality of life in other ways,” the Nationwide Children’s Hospital project summary says. “The overall impacts” of puberty blockers “have not been systematically studied,” the summary says.
One of the larger NIH-funded transgender studies, funded at $743,000 annually, is at Boston Children’s Hospital. It notes, “Little is known [emphasis added] about how pubertal blockade, the first step in the medical management of a young transgender adolescent, affects bone health and psychological well-being. … In an exploratory aim, we will also consider the effect of pubertal blockade on anxiety, depression, and health-related quality of life.”
Another research project, “Psychological consequences of medical transition in transgender youth,” begun last year at Princeton University and anticipated to end in 2025, notes the lack of quality research in this area:
Five studies to date have longitudinally examined the relationship between one or both of these interventions [puberty suppression and hormone therapy] and mental health in transgender youth. However, these studies have had relatively small samples, none have been able to isolate the effects of endocrine interventions, none have included a cisgender [non-transgender] comparison group, and none have examined the mechanisms by which endocrine interventions might improve mental health.
A longitudinal study that began in 2015 and will run through at least 2026 acknowledges, “Transgender children and adolescents are a poorly understood and a distinctly understudied population in the United States. … Continuing our current research is imperative to expand the scant evidence-base currently guiding the clinical care of TGD [transgender and gender diverse] youth and thus, is of considerable public health significance.”
As the summary of one ongoing NIH-funded research project on sex hormones’ effects on the developing brain says, “There is little to no empirical data guiding clinical practices” of cross-sex hormone therapy in early pubertal adolescents, “highlighting the need for further research to address the critical knowledge gap.” The research, funded at $3 million so far to Stanford University, “will provide a much-needed foundation for understanding the longitudinal impact of treatments that are already being used [emphasis added] in clinical settings.”
The project will elucidate “how sex hormone therapy alters sex-specific risk for disease … and [its] impact on neural networks implicated in psychiatric disorders.” The research proposed “has never been conducted in early pubertal adolescents,” the summary reads.
NIH Acknowledges Limited Evidence, FDA Hasn’t Approved
The NIH, the largest public funder of biomedical research in the world, told Reuters that “the evidence is limited on whether these treatments pose short- or long-term health risks for transgender and other gender-diverse adolescents.” Additionally, the Food and Drug Administration has not approved puberty blockers and sex hormones for children’s transgender medical interventions. As Reuters reported:
No clinical trials have established their safety for such off-label use. The drugs’ long-term effects on fertility and sexual function remain unclear. And in 2016, the FDA ordered makers of puberty blockers to add a warning about psychiatric problems to the drugs’ label after the agency received several reports of suicidal thoughts in children who were taking them. More broadly, no large-scale studies have tracked people who received gender-related medical care as children to determine how many remained satisfied with their treatment as they aged and how many eventually regretted transitioning.
Countries such as Finland, Sweden, and the United Kingdom have begun to limit children’s access to transgender health interventions. Early, foundational research from 2011 on transgender medical interventions has been criticized as failing to meet basic research standards.
Before 2012, “there was no scientific literature on girls ages eleven to twenty-one ever having developed gender dysphoria at all,” according to Abigail Shrier’s book “Irreversible Damage.” Studies show most children grow out of gender dysphoria, Shrier says.“There are no good long-term studies indicating that either gender dysphoria or suicidality diminishes after medical transition,” according to Shrier.
Meanwhile, despite all the possible health risks, President Joe Biden has issued executiveorders charging “HHS to work with states to promote expanded access to gender-affirming care.” The administration has issued directives that federal health insurance benefits must “provide comprehensive gender-affirming care.” The administration also opposes “conversion therapy — efforts to suppress or change an individual’s sexual orientation, gender identity, or gender expression.”
Taxpayers are already paying for transgender procedures, as they are covered by some insurers and Medicaid in some states.
I’ll ask again. WHY ARE THESE MENTAL PATIENT LEFTEST SO HYPER ABOUT MUTILATING AMERICA’S CONFUSED CHILDREN? WHAT IS THEIR END GAME?
HHS’s Office of Population Affairs, which is overseen by transgender Dr. Rachel Levine, states there’s no debate: “Research demonstrates that gender-affirming care improves the mental health and overall well-being of gender diverse children and adolescents.” Other proponents acknowledge a lack of research on these hormones’ effect on brain development, but say the pros outweigh the cons.
Growing Transgender Identification
The number of transgender adults in the U.S. is estimated at 1.4 million to 2 million, with an estimated 150,000 to 300,000 transgender children. The number of American children who started on puberty blockers or hormones totaled 17,683 from 2017 to 2021 and has been increasing, according to Reuters.
From 2019 to 2021, at least 56 patients ages 13 to 17 had genital surgeries, and from 2019 to 2021, at least 776 children that age had mastectomies, not including procedures that weren’t covered by insurance, according to Reuters.
The transgender surgery industry grosses more than $2 billion annually and expects to double that by 2030.
Debate Among Medication Providers
“Puberty delay medications are safe and effective,”according to the World Professional Association for Transgender Health (WPATH), a pro-transgender organization that sets standards for trans medical interventions. “Every person, including every TGD person, deserves an opportunity to be their true selves and has the right to access medically-necessary affirming care to enable this opportunity,” WPATH says.
When WPATH recently updated its guidance, authors “were acutely aware that any unknowns that the working group acknowledged — any uncertainties in the research — could be read as undermining the field’s credibility and feed the right-wing effort to outlaw gender-related care,” The New York Times reported. The newspaper is in the midst of an internal fight about its coverage of transgender issues, with some saying it has been too critical of transgender medical interventions.
A draft of the WPATH chapter for adolescents included minimum recommended ages for hormone treatments and breast removal or augmentation, but after criticism from providers and transgender activists, “it was determined that the specific ages would be removed to ensure greater access to care for more people,” WPATH said.
The final guidelines also walked back a recommendation that preteens and teenagers should provide evidence of several years of persistently identifying as transgender, to differentiate from kids whose change in identification is recent, and changed it to a vaguer “sustained” gender incongruence. “In the end, the chapter sided with the trans advocates who didn’t want kids to have to wait through potentially painful years of physical development,” according to the Times.
The final guidelines acknowledged that because of the limited long-term research, treatment without a comprehensive diagnostic assessment “has no empirical support and therefore carries the risk that the decision to start gender-affirming medical interventions may not be in the long-term best interest of the young person at that time.”
Reuters found that gender facilities across the country are not conducting recommended months-long assessments before administering hormones to children. Parents of 28 of 39 minors who had sought transgender interventions told Reuters they “felt pressured or rushed to proceed with treatment.” Gender-care professionals also said some of their peers are “pushing too many families to pursue treatment for their children before they undergo the comprehensive assessments recommended in professional guidelines.”
Studying Causes of Gender Dysphoria
Some of the taxpayer-funded studies may bring clarity to the issue of gender dysphoria by examining its causes. One study will examine social media’s influence on children becoming transgender. A second will study “the life history calendar to examine young transgender women’s trajectories of violence, mental health, and protective processes.”
Another government-funded study will help determine how chromosomes, sexual organs, and hormones combine to create sex differences. Another will “uncover genetic underpinnings of female sexual orientation.”
This byline marks several different individuals, granted anonymity in cases where publishing an article on The Federalist would credibly threaten close personal relationships, their safety, or their jobs. We verify the identities of those who publish anonymously with The Federalist.
Children in America are in need of protection now more than ever. The leftist tide is coming at them in full force, pushing a radically sexualized agenda on minors both mentally and physically, robbing them of their innocence and their childhood. That’s why legislators like Rep. Marjorie Taylor Greene, R-Ga., are introducing legislation to protect children from dangerous experimental procedures such as puberty blockers, wrong-sex hormones, and ill-named “gender-affirming” surgeries.
Instead of being allowed to enjoy the innocence of childhood, develop imagination, cultivate friendships, develop curiosity, and enjoy the satisfaction of learning facts, figures, and formulas, children are assaulted with sexualized content fueled by a radical agenda. If you think it’s not having an effect, just look at a sampling from Maryland schools. According to school surveys in Montgomery county, over the last two years, the number of students identifying as gender nonconforming has increased by 582 percent. This survey includes children in elementary school.
At the very least, parents should be fully aware of any and all exposure their children have to sexualized content, and they have the primary right to know of any confusion or distress their children may be experiencing in school. Yet somehow it is becoming more to push policies to keep parents in the dark. Most schools cannot even prescribe aspirin to a child without parental consent, yet they see no issue with socially transitioning a minor without parental involvement. The disparity gives every cause for concern.
And when the parents do know about their child’s gender confusion, the agenda becomes even more radical, pushing parents to “affirm” their child’s choices to extreme degrees. Whether you embrace the ideology, no amount of parental concern can justify even the slightest delay in transitioning a child.
Compliance, Not Concern
One lesbian couple had already transitioned their eldest son when their second boy started asking to be called a girl. Unlike their first child, who had preferred playing with girls and had a gentler side, the younger acted like a typical boy, so his mother suspected that he was simply mirroring his older sibling’s behavior. But what happened when she voiced her concerns to a gender therapist?
“She [their gender therapist] expressed that it was transphobic to believe there was anything wrong with our younger son wanting to be like his older transgender sibling. When I pushed back, and asserted that I was not yet convinced our younger son was transgender, she told me that if I did not change his pronouns and honor his identity, he could develop an attachment disorder,” the mom recalls.
Instead of addressing the mother’s fears, the therapist merely preyed on them further.
It’s horrible to emotionally blackmail loving parents while blatantly ignoring their genuine concerns, but this is mild compared to the psychological manipulation that’s been waged on other parents, who have been told “comply or they die,” with doctors insisting that any questioning of their child’s feelings will result in further depression and suicide.
Meanwhile, these “experts” are not basing their methods in science at all.
So Much for Science
According to the recent Heritage report, “Puberty Blockers, Cross-Sex Hormones, & Youth Suicide” by Dr. Jay Greene, stats show that the exact opposite may be the case. He writes, “Starting in 2010, when puberty blockers and cross-sex hormones became widely available, elevated suicide rates in states where minors can more easily access those medical interventions became observable.”
That’s right, here it seems that access to these “life-saving drugs” has actually increased suicide rates. The fact is, there is no golden standard study proving the “lifesaving” claims of transition, yet left-wing politicians insist that it is the only path forward.
There isproof that these drugs are dangerous on their own, and there is no certifiable data proving the long-term harmlessness of puberty-blocking drugs and wrong-sex hormones, despite leftist claims to the contrary.
This isn’t health care. This isn’t science. We need to stop using children to wage ideological warfare, and we must stop the progressive tide before every child pays the price.
A Reason for Hope
Rep. Taylor Green is trying to do just that. She recently released the Protect Children’s Innocence Act (H.R.8731), which, if passed, will charge anyone who knowingly performs “gender-affirming care” — including the administering of puberty blockers and wrong-sex hormones — with a class C felony.
The bill will prohibit the federal taxpayer funding of so-called gender-affirming care, forbid institutions of higher education from providing instructions on such care, and will prevent aliens who have performed such procedures from receiving a visa. If they already have a visa, they will be eligible for deportation. It is designed to protect children from abusive experimental procedures from every angle.
Victims of surgery who realize their mistake and choose to detransition have recourse to the courts through a private right of action levied against anyone who took an active part in their transition, including administering puberty blockers and performing surgeries. There is no statute of limitations, ensuring that anyone involved in destroying a child’s life will be held accountable in perpetuity.
This bill also looks out for those victims who have already suffered at the hands of misleading therapists, doctors, and propaganda. While it does ban transition attempts on minors, it explicitly states that it in no way prohibits doctors from helping patients handle complications due to those interventions, regardless of whether they were received illegally. In every aspect, this bill holds the health of these patients as its primary object, not monetary benefits and soul-sucking propaganda.
Fighting on defense in the culture isn’t enough. We’re losing — more and more children are being subjected to these horrific “treatments” every single day. We need to fight back legislatively. We need to protect the innocence of children and demand justice for those who have already been deprived of that privilege. If the battleground is in our backyard, this bill gives us the chance to push back enemy lines, to establish a first line of defense that will allow our children the space they need to grow and thrive.
The character of our country will be determined by whether we are willing to defend our innocents. Children being mutilated and castrated openly is the moral issue of our time. Will we stand up and fight? Or will we let these evil monsters continue to wreak havoc on the helpless?
Sandra Kirby is the Government Affairs Manager at American Principles Project. Follow her on Twitter @SandraK1776.
In less than one month, if Proposal 3 passes, children will have a right under the Michigan constitution to walk into one of Planned Parenthood’s 12 so-called “gender affirming” facilities in the state and, without parental knowledge or consent, obtain puberty blockers. And with Planned Parenthood of Michigan promising “gender affirming” care “via telehealth in the coming months,” Michiganders’ kids won’t even need to leave their house to obtain these sterilizing drugs.
Passage of Prop 3 will also give boys a constitutional right to be castrated and girls the right under Michigan’s constitution to be sterilized by way of a hysterectomy or the removal of their ovaries — all without their parents’ consent.
Deceptive marketing by Planned Parenthood and far-left politicians, such as Gov. Gretchen Whitmer, hides this reality from Michigan voters, leading Prop 3 to be uniformly referred to as “the abortion amendment” even though the expansive language of the proposed constitutional amendment reaches far beyond abortion. And on abortion alone, notwithstanding proponents’ claims that “passing this amendment simply restores the same protections that Michiganders had for five decades under Roe v. Wade,” Prop 3 goes far beyond the controlling Roe-Casey precedent: If passed, the constitutional amendment would create an extreme regime in Michigan of abortion on demand, at any time, for any reason, without informed or parental consent, and paid for by taxpayers.
The expansive and legalistically worded language of Prop 3, crafted by Planned Parenthood and left-wing backers, however, extends beyond abortion to create a constitutional right to several aspects of what transgender activists call “gender-affirming care,” despite it being neither affirming nor caring. And Prop 3 extends that right to all individuals, including children.
This is not merely a political point, and it is not a worst-case-scenario argument based on how some liberal activist judge or justice might interpret Prop 3. This reality flows from the plain language of Prop 3 and rests on general legal principles of constitutional construction.
It’s Right in the Text
Here is the pertinent language Prop 3 would etch into the Michigan constitution as Article 1, Section 28, with the key language underscored:
“(1) Every individual has a fundamental right to reproductive freedom, which entails the right to make and effectuate decisions about all matters relating to pregnancy, including but not limited to prenatal care, childbirth, postpartum care, contraception, sterilization, abortion care, miscarriage management, and infertility care. An individual’s right to reproductive freedom shall not be denied, burdened, nor infringed upon unless justified by a compelling state interest achieved by the least restrictive means. …
(2) The state shall not discriminate in the protection or enforcement of this fundamental right.
* * *
(4) For the purposes of this section:
A state interest is “compelling” only if it is for the limited purpose of protecting the health of an individual seeking care, consistent with accepted clinical standards of practice and evidence-based medicine, and does not infringe on that individual’s autonomous decision-making.
* * *
(5) This section shall be self-executing….
Prop 3 Applies to Men and Women AND Boys and Girls
By its express terms, Prop 3 applies to “every individual” and guarantees an “individual’s right.” The proposed constitutional amendment further provides that “the state shall not discriminate in the protection or enforcement of this fundamental right.”
As a matter of constitutional interpretation, then, the rights guaranteed by Prop 3 would be rights that both adults and children possess as “individuals,” and the rights apply equally to males and females.
This proposal represents a huge demarcation from controlling Michigan law, under which minors must have parental consent to obtain medical treatment or receive prescription medications, with the only current exception being the judicial bypass provisions governing minors seeking abortions. Specifically, Michigan law currently provides that to obtain an abortion, females under the age of 18 must have the written consent of one parent or legal guardian, but the law allows a girl to seek permission for an abortion from a judge, called a “judicial bypass.” A court must grant a judicial bypass if the judge finds either that “the minor is sufficiently mature and well-enough informed to make the decision regarding abortion independently of her parents or legal guardian,” or “the waiver would be in the best interests of the minor.”
In the context of abortion, Prop 3 guts Michigan’s requirements for either parental consent or a judicial bypass, first by declaring that the amendment applies to all “individuals” and second by expressly providing that “the state shall not discriminate in the protection or enforcement of this fundamental right.” Treating females under 18 differently than those 18 or over is a textbook example of discrimination.
Section 4 of the amendment further cements the reality that minors must be treated equivalent to adults for purposes of the rights Prop 3 would establish. That section of the proposed amendment expressly limits the justifications allowed for regulating abortion or the other rights Prop 3 would inscribe in the constitution.
Under Section 4, the state may only regulate abortion and the other rights covered by the proposed constitutional amendment if it is necessary to “protect[] the health of an individual seeking care,” and “does not infringe on that individual’s autonomous decision-making.”
The rights of parents do not matter; Mom and Dad have no rights. And even the health of the girl does not matter because, under the plain language of the amendment, the state’s interest cannot “infringe” on the “individual’s autonomous decision-making.”
This legal analysis flows straight from the plain language of Prop 3, but case law from other states where a state constitutional right to abortion exists confirms this analysis. For example, in Alaska and Florida, courts have declared parental consent and parental notification statutes unconstitutional. And courts in California, Massachusetts, and New Jersey have struck parental consent statutes.
Prop 3’s grant of such “autonomous decision-making” is not limited to abortion, however. Rather, the plain language of the proposed constitutional amendment provides that the right to “reproductive freedom,” “entails the right to make and effectuate decisions about all matters relating to pregnancy, including but not limited to … sterilization … or infertility care.”
Under Michigan law currently, minors cannot be chemically or surgically sterilized (or rendered infertile) without their parents’ consent, and even then most physicians would refuse to sterilize a minor — except in the case of transgender-identifying patients.
The modern medical community has embraced the transgender ideology that teaches that human beings can be born “in the wrong body,” and that the appropriate treatment for such individuals consists of making their bodies appear to conform to their “internal sense” of gender.
The first step in such wrongly named “gender-affirming” medical response consists of prescribing puberty blockers to children. Puberty blockers, at a minimum, render children temporarily infertile by preventing them from maturing sexually, and a longer-term use renders them sterile. The surgical procedures used under the guise of “gender confirmation” — castration, hysterectomy, and the removal of ovaries — likewise sterilize the patients.
In fact, it is this very destruction of children’s future fertility and the medical rendering of them sterile that has led to several states banning the use of puberty blockers and surgical “gender confirming” procedures on minors. For instance, in Iowa, the Legislature made these legislative findings to explain its proposed ban on puberty blockers and surgical procedures that sterilize children:
Puberty blockers prevent gonadal maturation and thus render children taking these drugs infertile. Introducing cross-sex hormones to children with immature gonads as a direct result of pubertal blockade is expected to cause irreversible sterility. Sterilization is also permanent for those who undergo surgery to remove reproductive organs[.] … For these reasons, the decision to pursue a course of hormonal and surgical interventions to address a discordance between an individual’s sex and sense of gender identity should not be presented to or determined for children who are incapable of comprehending the negative implications and life-course difficulties resulting from these interventions.
But in Michigan, if passed, Prop 3 guarantees children the right to “make and effectuate decisions about all matters relating to … sterilization,” and without “discrimination,” giving boys and girls the right to obtain puberty blockers and surgical sterilization without parental notice or consent.
If passed, Section 4 of the proposed constitutional amendment will further guarantee that the Michigan Legislature cannot interfere in transgender minors’ decisions to obtain puberty blockers or surgical “gender reassignment” through castration, removal of ovaries, or a hysterectomy. That section, as excerpted above, provides that the state may only regulate such procedures for the limited purpose of “protecting the health of an individual seeking care, consistent with accepted clinical standards of practice and evidence-based medicine,” and then, only so long as it “does not infringe on that individual’s autonomous decision-making.”
But the “accepted clinical standards of practice” by the supposed “mainstream” medical organizations is, at a minimum, to provide puberty blockers to children, with a steady movement toward the cash cow that is surgical interventions for minors.
Planned Parenthood Targets Kids One Way or Another
Again, these conclusions flow directly from the plain language of the proposed constitutional amendment. But here the public would be wise to note two significant facts: Planned Parenthood Advocates of Michigan helpedlead the ballot initiative to amend the Michigan constitution through the passage of Prop 3, deceptively described as the “Reproductive Freedom for All” amendment, and Planned Parenthood nowrepresents “the second largest provider of ‘gender-affirming hormone therapy.’” In fact, less than two weeks ago, Planned Parenthood launched an ad marketing puberty blockers to minors.
What Planned Parenthood and its extremist political partners don’t want publicized, however, is that a “Yes” vote for Prop 3 will not merely make abortion-on-demand, for any reason, at any time, and without informed or parental consent the law of Michigan: It will guarantee that children have an unfettered “right” to “transition” by obtaining puberty blockers and surgical sterilization, parents be damned.
With less than one month to go before Michiganders cast their final ballots, little time remains to give proof to the left’s lie that Prop 3 is about codifying Roe. It is not. It is about sacrificing the children of the state — both born and unborn.
Margot Cleveland is The Federalist’s senior legal correspondent. She is also a contributor to National Review Online, the Washington Examiner, Aleteia, and Townhall.com, and has been published in the Wall Street Journal and USA Today. Cleveland is a lawyer and a graduate of the Notre Dame Law School, where she earned the Hoynes Prize—the law school’s highest honor. She later served for nearly 25 years as a permanent law clerk for a federal appellate judge on the Seventh Circuit Court of Appeals. Cleveland is a former full-time university faculty member and now teaches as an adjunct from time to time. As a stay-at-home homeschooling mom of a young son with cystic fibrosis, Cleveland frequently writes on cultural issues related to parenting and special-needs children. Cleveland is on Twitter at @ProfMJCleveland. The views expressed here are those of Cleveland in her private capacity.
The nation’s public-health establishment lost all credibility during the Covid era by either ignoring or politicizing scientific data. But health bureaucrats seem to have learned nothing. With respect to the highly charged issue of gender dysphoria, they continue to substitute politics for science when necessary to advance the leftist narrative.
The Department of Health and Human Services (HHS) recently released an official document designed to enshrine experimental medical interventions as the standard treatment for transgender-identifying children. Prepared by HHS’s Office of Population Affairs (OPA), the document is a political statement unmoored from actual medical research.
According to “Gender-Affirming Care and Young People,” medical interventions such as puberty-blocking drugs, wrong-sex hormones, and surgical mutilation are “crucial to overall health” of young people confused about their sex. (For what it’s worth, OPA falls under the supervision of Dr. Rachel Levine, a man who identifies as a woman.) The document complements a proposed rule announced by HHS in March, mandating insurance coverage for such “gender-affirming care.”
But the claims made in HHS’s new release have been deftly dismantled by an organization of physicians and scientists who still care about reality, and about ethical medical practice. The Society for Evidence Based Gender Medicine (SEGM) — which exists “to promote safe, compassionate, ethical and evidence-informed healthcare for children, adolescents, and young adults with gender dysphoria”—points out that HHS’s discussion is deeply misleading and indeed dangerous. SEGM identifies seven serious misrepresentations of fact crammed into the two-page HHS document. Most of these involve cherry-picking, distorting, or simply ignoring the results of studies on the many facets of so-called gender-affirming treatment.
HHS Mischaracterizes Studies
For example, HHS flatly mischaracterizes a study that failed to find any benefits of “social transition” (presenting oneself as the opposite sex, with a new name, hairstyle, dress, etc.). As SEGM notes, the HHS document cites that study for the opposite conclusion, “wrongly assert[ing] that social transition improves functioning.” HHS presumably assumes readers won’t read the actual study and thus will accept the agency’s false claims about its findings.
SEGM identifies other falsifications of the supposed mental-health benefits of wrong-sex hormones and surgeries. HHS’s “claims of benefits coming from cherry-picked studies do not hold up when the entire body of evidence is properly evaluated in a systematic and reproducible way,” according to SEGM.
The design of the studies cited by HHS made it impossible to link medical interventions and improved mental health, SEGM observes. By contrast, multiple European studies “concluded that there is a lack of convincing evidence for the mental health benefit for children and adolescents of either puberty blockers or cross-sex hormones.”
SEGM notes, in fact, that the Swedish health authority warned that “the risks of puberty suppressing treatment . . . and gender-affirming hormonal treatment currently outweigh the possible benefits, and that the treatments should be offered only in exceptional cases.”
HHS ignored all this research, which would have led honest medical professionals to at least acknowledge the scholarly debate about the wisdom of these interventions. But HHS isn’t run by honest medical professionals. It’s in the grip of ideologues determined to drive troubled children and their families into the clutches of the trans industry.
Dishonest Use of Data on Suicide
SEGM also criticizes the HHS document for dishonesty about the related issue of suicide among trans-identifying youth. In claiming alarmingly high rates of suicidal ideation in this population — a claim routinely used to pressure desperate parents into consenting to dangerous medical interventions — HHS relies only on “a low quality, non-probability online survey.”
In fact, SEGM reports, “recent research from one of the world’s largest pediatric gender clinics estimated the rate of suicide in trans-identified youth as 0.03% over a 10-year period, which is comparable to youth presenting for care with mental health problems.”
Even more critically, despite HHS’s strong implication that drugs, hormones, and surgeries reduce suicide rates, SEGM clarifies that “no study to date has demonstrated that transition reduces the rate of serious suicide attempts.” Is HHS afraid that telling the truth about suicide will make parents less likely to place their troubled children on the trans-industry conveyor belt?
Puberty Blockers Are Not Fully Reversible
The mendacity of HHS extends beyond misrepresenting or ignoring studies. For example, the document states, without supporting citation, that puberty blockers are fully reversible (i.e., natural puberty will resume once the drugs are discontinued). But SEGM warns about the utter dearth of research supporting this claim. In fact,
concerns have been raised that puberty blockers are psychologically irreversible (since over 95% of all treated youth proceed to cross-sex hormones), that they may harm bone development, may permanently alter the brain, that it is not yet known how they affect other vital organs, all of which undergo significant structural changes during uninterrupted puberty.
Once again, public-health agencies in Europe are more honest. As SEGM reports, Britain’s National Health Service says that “[l]ittle is known about the long-term side effects of hormone or puberty blockers in children with gender dysphoria.”
But ignoring the risks of these interventions is HHS’s modus operandi. SEGM calls out the HHS ideologues for mentioning only the supposed (in some cases imaginary) benefits of interventions while failing to mention documented risks to bone development, cardiovascular health, and the mental health of patients who later regret their transition decisions.
Sterility Expected After Trans Treatments
SEGM particularly targets HHS’s failure to mention the effect on reproductive health, which is supposed to be the focus of Levine’s Office of Population Affairs. “When puberty blockers are administered in early puberty and followed by cross-sex hormones,” SEGM notes, “sterility is expected.”
HHS is silent about this potentially devastating consequence. Nor does it acknowledge the “serious ethical questions about whether adolescents can be considered competent to waive their future reproductive rights at an age when they are unlikely to be able to appreciate or predict the importance of fertility to their adult selves.”
Ethics, it appears, is not HHS’s strong suit.
HHS also misleads in stating that mutilating surgeries are “typically used in adulthood or case-by-case in adolescence.” In fact, as SEGM notes, draft recommendations from the influential (though highly politicized) World Professional Association for Transgender Health (WPATH) urge broad availability of mastectomies to patients at age 16.
Even worse, patients as young as 13 had their healthy breasts removed as part of a study funded by the National Institutes of Health – i.e., by you and me through our tax dollars. The HHS bureaucrats who prepared this report surely knew this, but distort the facts.
This HHS document, then, is a farce. As SEGM summarizes, HHS inadequately reviewed the scientific literature, issued “biased recommendations that do not acknowledge the low quality of evidence,” failed to solicit input from professionals and patients whose experiences contradict the government narrative, and utterly ignored possible alternatives to medical interventions, such as psychotherapy. The result:
This incomplete representation of the relevant issues is likely to mislead the public to believe that this is the best and only alternative, particularly when no other alternatives are mentioned. The public is also likely to erroneously assume that the risks of affirmative care are low. Patients and families are not capable of providing valid informed consent when the information they receive is inaccurate and incomplete
If the public-health establishment wants to rehabilitate its tattered reputation after the Covid debacle, this isn’t the way to do it. Health policy is too important to be entrusted to political hacks.
Jane Robbins is an attorney and a retired senior fellow with the American Principles Project in Washington DC. In that position she crafted federal and state legislation designed to restore the constitutional autonomy of states and parents in education policy, and to protect the rights of religious freedom and conscience. She is a graduate of Clemson University and the Harvard Law School.
President Joe Biden declared his support for allowing children and adolescents with gender dysphoria to undergo body mutilating surgeries or use puberty blockers and cross-sex hormones to look more like the opposite sex despite unknowns about longterm side effects. In multiple documents released Thursday, which is observed by some as the Transgender Day of Visibility, the Biden administration backed what it described as “gender-affirming health care” for children.
The document states that “early gender-affirming care” for non-binary or trans-identified minors “is crucial to overall health and well-being as it allows the child or adolescent to focus on social transitions and can increase their confidence while navigating the healthcare system.”
The document lists “top” surgeries — elective mastectomies and breasts enhancements — and “bottom” surgeries — removal of genitals — as “gender-affirming care.”
The document states that the surgeries are “[t]ypically used in adulthood or case by-case in adolescence.”
“Gender-affirming care is a supportive form of healthcare. It consists of an array of services that may include medical, surgical, mental health, and non-medical services for transgender and nonbinary people,” stated OPA.
“Medical and psychosocial gender affirming healthcare practices have been demonstrated to yield lower rates of adverse mental health outcomes, build self-esteem, and improve overall quality of life for transgender and gender diverse youth.”
HHS’ Substance Abuse and Mental Health Services Administration’s National Child Traumatic Stress Network released a document titled “Gender-Affirming Care Is Trauma-Informed Care.”
The network’s document defined gender-affirming care as including so-called “evidence-based interventions such as puberty blockers and gender-affirming hormones” and proclaimed that “gender-affirming care is neither child maltreatment nor malpractice.” The statement comes as officials in Texas have defined administering puberty-blocking drugs on children who question their gender as “child abuse” and experimental since the Food and Drug Administration has not approved such drugs for that use.
“There is no scientifically sound research showing negative impacts from providing gender-affirming care,” the network’s statement adds. “[Transgender, gender diverse, and intersex] youth can thrive when they are supported and affirmed in their identities and their identity development.”
An entry on Mayo Clinic’s website states that drugs aimed at blocking puberty “might” help reduce depression among youth. “However, puberty suppression alone might not ease gender dysphoria,” said the clinic, adding, Using medication to delay puberty “beyond one’s peers can be stressful,” and thus, a child “might experience lower self-esteem.”
The conservative American College of Pediatricians, an association of physicians and healthcare professionals “dedicated to the health and well-being of children,” has long voiced its opposition to using puberty-blocking drugs on children suffering from gender dysphoria.
“There is not a single long-term study to demonstrate the safety or efficacy of puberty blockers, cross-sex hormones and surgeries for transgender-believing youth,” the organization said in a statement.
“This means that youth transition is experimental, and therefore, parents cannot provide informed consent, nor can minors provide assent for these interventions. Moreover, the best long-term evidence we have among adults shows that medical intervention fails to reduce suicide.”
“Temporary use of puberty blocker Lupron has also been associated with and may be the cause of many serious permanent side effects including osteoporosis, mood disorders, seizures, cognitive impairment and, when combined with cross-sex hormones, sterility,” the American College of Pediatricians added. “In addition to the harm from Lupron, cross-sex hormones put youth at an increased risk of heart attacks, stroke, diabetes, blood clots and cancers across their lifespan.”
The American Academy of Pediatrics has issued medical guidelines that supportthe surgical and hormonal transition of trans-identified children and adolescents.
“Often, pubertal suppression creates an opportunity to reduce distress that may occur with the development of secondary sexual characteristics and allow for gender-affirming care, including mental health support for the adolescent and the family,” an October 2018 AAP guideline states.
Supporters of puberty blockers have long claimed that puberty blockers’ impact on children is reversible and are designed to give children with gender dysphoria more time to decide which gender they identify as. Proponents also claim that once adolescent users stop taking puberty blockers, their puberty resumes. The new OPA document claims that puberty blockers are reversible.
However, the United Kingdom’s National Health Service reports that “[l]ittle is known about the long-term side effects of hormone or puberty blockers in children with gender dysphoria.”
“Although GIDS advises this is a physically reversible treatment if stopped, it is not known what the psychological effects may be,” the NHS website explains. “It’s also not known whether hormone blockers affect the development of the teenage brain or children’s bones. Side effects may also include hot flushes, fatigue and mood alterations.”
As teens who are 16 or over and have been on puberty blockers for at least a year are eligible to start cross-sex hormones in the U.K., the NHS warns that those “hormones cause some irreversible changes,” such as breast development and deepening of the voice.
“Long-term cross-sex hormone treatment may cause temporary or even permanent infertility,” the NHS website added. “There is some uncertainty about the risks of long-term cross-sex hormone treatment.”
The state of Texas has made headlines in the last year as Gov. Greg Abbott, Attorney General Ken Paxton and the state’s child services agency have questioned whether prescribing puberty-blocking drugs and cross-sex hormones to minors could constitute “child abuse.” In February, Paxton issued a formal opinion stating that prescribing puberty blockers or conducting sex-change surgeries on children with gender dysphoria “can legally constitute child abuse under several provisions of chapter 261 of the Texas Family Code.” Texas is also investigating whether AbbVie Inc. and Endo Pharmaceuticals, Inc., manufacturers of puberty blockers, have been engaging in deceptive advertising practices. Paxton’s office had issued Civil Investigative Demands against the two companies, seeking to determine “whether these manufacturers of puberty-blocking drugs deceptively advertised and promoted hormone blockers for unapproved uses without disclosing the potential risks to children and their parents.”
“Companies should never promote or supply puberty blockers for uses that are not intended or approved,” stated Paxton. “I will not allow Big Pharma to misleadingly promote these drugs that may pose a high risk of serious physical and psychological damage to Texas children who cannot yet fathom or consent to the potential long-term effects of such use.”
The Biden administration has challenged Texas, with the president claiming that his administration is putting “Texas on notice that their discriminatory actions put children’s lives at risk.” The administration issued guidelines saying that it may violate federal law for Texas to charge doctors who administer gender reassignment surgeries or puberty blockers on children with “child abuse.”
Earlier this month, Paxton sued the Department of Health and Human Services and argued that the federal government is misinterpreting federal law and that Texas law does allow him to label such acts as “child abuse.” A state appellate court struck down Abbott’s directive instructing the Texas Department of Family and Protective Services to “conduct a prompt and thorough investigation of any reported instances of these abusive procedures.”
The attorney general’s office has asked the Texas Supreme Court to reverse the lower court decision blocking the directive.
As a result of the governor’s directive and attorney general’s opinion, the Houston-based Texas Children’s Hospital stated earlier this month that it will pause “hormone-related prescription therapies for gender-affirming services.”
The transgender misinformation machine is at it again. The New York Times recently published an extensive essay arguing against screening before medical transition — if someone says she wants hormones or surgery, doctors should immediately break out the syringes and prep the operating room.
The article, by Alex Marzano-Lesnevich of Bowdoin College, exemplifies how the transgender movement uses misinformation to advance its agenda. Marzano-Lesnevich asserts, “That gender-affirming health care saves lives is clear: A 2018 literature review by Cornell University concluded that 93 percent of studies found that transition improved transgender people’s heath [sic] outcomes, while the remaining 7 percent found mixed or null results. Not a single study in the review concluded negative impact.”
That seems dispositive — unless you look at the studies. The cited literature review was titled the “What We Know Project” and was directed by the LGBT scholar and activist Nathaniel Frank, who cited it in his own New York Times piece on transgenderism a few years ago, writing that “Our findings make it indisputable that gender transition has a positive effect on transgender well-being.”
Poorly Conducted Studies
These proclamations that the science is settled are a bold facade on rickety scaffolding. When this New York Times article invokes the authority of science, it seeks to evoke the image of careful statisticians sifting through data collected by diligent doctors.
But it is actually appealing to self-selected online surveys with cash prizes, studies with tiny samples, and studies that are missing more than half of their subjects. Stacking a bunch of weak studies on top of each other doesn’t provide a strong result, but The New York Times presumes readers won’t bother to check the details — the editors certainly didn’t.
Back in 2019, I took a closer look at the studies the What We Know Project cites, and found a methodological mess. Many of the studies had serious flaws, beginning with small sample sizes. As I noted, “Of the fifty relevant papers identified by the project, only five studies (10 percent) had more than 300 subjects, while twenty-six studies (52 percent) had fewer than 100. Seventeen studies (34 percent) had fifty or fewer subjects, and five of those had a sample size of twenty-five or less.”
The flaws extended far beyond small sample size, and the largest studies tended to be the weakest, often consisting of little more than online surveys with a self-selecting sample. Nor should we put much faith in a study that recruited subjects for an online survey by advertising “on online groups and discussion forums that were dedicated to FTM [female-to-male] members. . . . Upon survey completion, participants were entered into a lottery drawing for cash prizes.”
Even the better-designed long-term studies were often plagued by poor response rates. A European study had 201 out of 546 respond — just 37 percent. And though missing data is, by definition, missing, it is reasonable to suspect that those with poor outcomes are overrepresented among those who could not or would not respond.
Regret Rates
Nor did The New York Times check Marzano-Lesnevich’s claim that “gender-affirming health care has some of the lowest rates of regret in medicine. A 2021 systemic review of the medical literature, covering 27 studies and 7,928 transgender patients, found a regret rate of 1 percent or less.” But read the paper and it is quickly apparent both that the review has significant weaknesses and that The New York Times allowed its conclusions to be misrepresented.
Of the 27 studies used in their analysis, the review authors ranked only five as “good” and only four as having a low risk of bias. Many of the studies had the same flaws as those examined in the What We Know Project (indeed, some studies were used in both).
Another problem is that the majority of the data in the 2021 review came from a single study conducted by a Dutch group retrospectively examining the records of their own gender clinic. But a retrospective review of medical files will only identify regrets from patients who shared them with the gender clinic that performed their surgeries. Furthermore, the study only identified regrets following gonadectomy, and not those who regretted other surgeries, or who never had surgery but did regret taking cross-sex hormones or puberty blockers.
In addition to the problem of allowing a flawed data set to dominate the 2021 review, this illustrates another persistent difficulty with studies of transgender regret, which is that they are often conducted by those who provide medical transition, rather than independent researchers. People whose livelihoods and reputations depend on facilitating medical transition might be less than diligent and rigorous in looking for regret.
To their credit, the authors of the 2021 review do discuss some of the limits and difficulties of their work, writing that various problems:
represent a big barrier for generalization of the results of this study. The lack of validated questionnaires to evaluate regret in this population is a significant limiting factor. In addition, bias can occur because patients might restrain from expressing regrets due to fear of being judged by the interviewer. Moreover, the temporarity of the feeling of regret in some patients and the variable definition of regret may underestimate the real prevalence of ‘true’ regret.
None of these qualifications regarding regret were even hinted at in the published column. Despite The New York Times’ citing it, the 2021 review does not prove that “gender-affirming health care has some of the lowest rates of regret in medicine.”
As the authors note, regret is not only an imperfect measure, but it is often difficult to measure, with no set criteria defining it. In one Swedish review cited by the What We Know Project, it was defined “as application for reversal of the legal gender status among those who were sex reassigned,” which excludes those who succumbed to depression or addiction, or who lived unhappily after transition without seeking to legally detransition.
Gatekeeping before Transition
Furthermore, even if we uncritically accept the results of the 2021 review, it does not support the argument that gatekeeping before medical transition is unnecessary and harmful. Rather, the authors claim that the low regret rate they found “reflects and corroborates the increased [sic] in accuracy of patient selection criteria for GAS [gender affirmation surgery].”
In short, the review argues that medical gatekeeping keeps regret rates low. That The New York Times allowed this review to be used as evidence against medical screening, and in favor of self-ID for medical transition, exemplifies the persistent practice of American transgender activists using studies of (mostly) carefully screened European adults to argue against screening before medical transition, even for children.
Unfortunately, the aggregation of (often questionable) studies, and the exaggeration of their conclusions by activists, is only part of the problem. These efforts to spread misinformation are augmented by the intimidation of dissenting scientists and the suppression of results that trans activists dislike.
Suppressing Dissent
Researchers have learned to fear the wrath of LGBT activists, and take pains to avoid it. Results that undermine the narrative have to be carefully presented lest the public draw the wrong conclusions. Thus, when scientists concluded that there is no “gay gene” they “worked with LGBTQ advocacy groups and science-communication specialists on the best way to convey their findings in the research paper and to the public.”
With regard to transgender ideology, the intimidation is even more overt. For example, Lisa Littman’s qualitative study describing the phenomenon of rapid-onset gender dysphoria met a ferocious response from transgender activists. Similarly, activists smeared Canadian psychologist Kenneth Zucker and forced him out of his position as the leader of a gender identity clinic, even though he sometimes supported transitioning children. He was just more cautious about it than activists wanted. He was eventually vindicated, but targeting him still sent a warning to any researchers who are seen as insufficiently pro-trans.
As these cases demonstrate, the science is being manipulated to fit transgender ideology. Shoddy studies — often conducted by activists and doctors with a stake in medical transition — are boosted if they support the trans narrative, while results and researchers who challenge it are suppressed. This skewed data is then used by trans activists and their allies to shape the discourse.
Uncomfortable facts and stories are kept out of the official narrative. Insightful and moving first-person accounts of transition and detransition are confined to non-traditional outlets such as Substack, as are the warnings of leading trans doctors about the reckless rushing of children into transition. The information bubble is the point.
Going forward, disagreement will be labeled “misinformation” and banned from social media, and dissidents will be labeled as bigots who should be fired from their jobs. Doctors will be required to practice only according to the approved narrative, and educators will encourage children to transition without parental knowledge and consent. Worse still, the government will take children from parents who do not support transition.
The purpose of the transgender misinformation machine is not so much to persuade, but to provide justification for coercion. The point of the lies and distortions is to impose transgender ideology on all of us, especially children.
Nathanael Blake is a senior contributor to The Federalist and a postdoctoral fellow at the Ethics and Public Policy Center.
Events happened this year that would have been believed impossible not long ago, with new lows and technological advances.
The world seemed to get closer to spinning out of its orbit in 2021. If you’d told me five years ago that men would be treated as women, criminals would not be prosecuted, and censorship would be widespread, I wouldn’t have believed you.
What were once considered the most basic, scientific truths (such as that you’re born with your sex and can’t change it) have broken down. Governments are no longer serving their primary function of providing security and protecting borders.
There are many more. As I reflected on the past year, here are just some of the many things that happened in 2021 that I never would have believed possible if someone had foretold them to me just five years ago.
1. Men As Women
The trend that most would have shocked my grandparents is transgenderism. Men are now competing with women in sports and being housed with women in prison. In 2021, President Biden appointed a man as a four-star admiral and proclaimed this was the “first” “female” “four-star officer.”
2. Blocking Puberty
A second shocker is that parents are enabling young children to try to change genders with dangerous surgeries and puberty blockers. Many public schools have a policy of not telling parents if their son or daughter has adopted a transgender identity at school.
3. Drafting Women
Third, the United States narrowly avoided a draft for women, which was supported by many elected officials in the “conservative” party.
Millions of immigrants have crossed illegally into the United States this year, in record numbers. The Biden administration also considered paying $450,000 in reparations to illegal immigrant families separated at the border.
6. Widespread Censorship
The former president of the United States is still banned from Facebook and Twitter. Big Tech censors debate on the most important topics of the day. Comedians can’t make jokes.
7. Parents Labeled Terrorists
Parents were labeled “domestic terrorists” by the Biden Justice Department for showing up at school board meetings with complaints. Schools aren’t telling parents what they teach and politicians are denying the obvious – young children are being taught, using public funds and institutions, that their country is racist.
8. President’s Mental Abilities Doubted
President Biden misspeaks regularly, to the point that many commentators doubt he’s really the one running the country.
9. Asking Athletes for Advice
People turn to athletes and actors more and more for their advice and opinions as many other societal leaders seem to have abdicated their duties to lead.
10. Record Debt and Inflation
With record U.S. national debt, the money supply increased by more than a third in 18 months. The United States is experiencing the worst inflation in 40 years. Energy prices are up, and one of the bigger events of the year was in May, when the main pipeline carrying gasoline to the East Coast was shut down due to a cyberattack.
11. Covid Restrictions Continue and Some Increase
Initially sold as “two weeks to slow the spread,” lockdowns, mask, and vaccine mandates continue two years since COVID-19 started. Some U.S. cities such as Los Angeles, New York, and Washington D.C. are now segregating people from public places to penalize their independent assessment of their medical risks.
12. Major Scientific Advances Not Celebrated
Every year brings some surprises and new scientific advances, but this year, living in a time of such great division in society, these breakthroughs were not universally celebrated.
Surely the greatest impact of science this year was the widespread rollout of COVID-19 vaccines. Thankfully, the vaccines have saved countless lives. But many had hoped they would mean life could return to normal; instead, lockdowns and mask mandates continue and vaccines have become yet another point of division, with the vaccinated pitted against the unvaccinated.
A huge portion of the world’s population has been willing to get the jab and trust relatively new Messenger RNA (mRNA) vaccines, but some have been doubtful and resisted coercion and mandates as they have made their own judgments about natural immunity and risk. According to the Centers for Disease Control, “mRNA vaccines are newly available to the public. However, researchers have been studying and working with mRNA vaccines for decades.”
Doubts have been sown because the vaccines don’t completely prevent infection or transmission, but also because the public has lost faith in science as it was politicized by scientists, the administration, bureaucrats, the media, and Big Tech – from discussion of the origins of COVID to its treatment and prevention.
Surely we could at least joyfully celebrate science when the long-time human dream of private space travel became more of a reality in 2021? Three billionaires made expeditions to this frontier. It was a massive milestone, but was criticized by some as a waste of money and an ego trip.
13. Losing Our Lead
While traveling to space sure sounds sci-fi, the United States is losing its lead in science. China continued its advances toward surpassing the United States in technology, surprising U.S. officials by launching a supersonic missile capable of carrying a nuclear warhead. The missile circled the earth once and barely missed its target.
It “approached its target traveling at least five times the speed of sound — a capability no country has previously demonstrated,” according to The Financial Times. The Pentagon is unsure how “China overcame the constraints of physics by firing countermeasures from a vehicle travelling at hypersonic speeds.”
China may also be behind some of the Unidentified Flying Objects seen by U.S. military pilots over the past two decades, according to a long-awaited Pentagon report this year, which could not explain the origin of the UFOs.
Even with all this bad news, our nation has so much to be grateful for. But looking at the societal chaos and dystopian scientific advances, it’s no wonder some think the end is nigh. For now, we can hope that Republican wins last November show that many Americans will vote for change in the next election.
And maybe we should celebrate those billionaires escaping Earth after all.
Eleanor Bartow is the features editor at The Federalist. She worked as an editor at The Daily Caller and an investigative reporter at the Daily Caller News Foundation. She was editor-in-chief of the American Enterprise Institute’s magazine, The American, and a reporter for Congressional Quarterly. Her articles have also been published with The New York Times, The Washington Post, Real Clear Investigations, National Geographic News, The International Herald Tribune, and The American Spectator. She has been interviewed on Fox News Radio, National Public Radio, and WABC. She received a Fulbright Professional Grant in Journalism and was a fellow with the Claremont Institute and National Review Institute.
American Family Association
American Family Association (AFA), a non-profit 501(c)(3) organization, was founded in 1977 by Donald E. Wildmon, who was the pastor of First United Methodist Church in Southaven, Mississippi, at the time. Since 1977, AFA has been on the frontlines of Ame
NEWSMAX
News, Opinion, Interviews, Research and discussion
Opinion
American Family Association
American Family Association (AFA), a non-profit 501(c)(3) organization, was founded in 1977 by Donald E. Wildmon, who was the pastor of First United Methodist Church in Southaven, Mississippi, at the time. Since 1977, AFA has been on the frontlines of Ame
American Family Association
American Family Association (AFA), a non-profit 501(c)(3) organization, was founded in 1977 by Donald E. Wildmon, who was the pastor of First United Methodist Church in Southaven, Mississippi, at the time. Since 1977, AFA has been on the frontlines of Ame
You Version
Bible Translations, Devotional Tools and Plans, BLOG, free mobile application; notes and more
Political
American Family Association
American Family Association (AFA), a non-profit 501(c)(3) organization, was founded in 1977 by Donald E. Wildmon, who was the pastor of First United Methodist Church in Southaven, Mississippi, at the time. Since 1977, AFA has been on the frontlines of Ame
NEWSMAX
News, Opinion, Interviews, Research and discussion
Spiritual
American Family Association
American Family Association (AFA), a non-profit 501(c)(3) organization, was founded in 1977 by Donald E. Wildmon, who was the pastor of First United Methodist Church in Southaven, Mississippi, at the time. Since 1977, AFA has been on the frontlines of Ame
Bible Gateway
The Bible Gateway is a tool for reading and researching scripture online — all in the language or translation of your choice! It provides advanced searching capabilities, which allow readers to find and compare particular passages in scripture based on



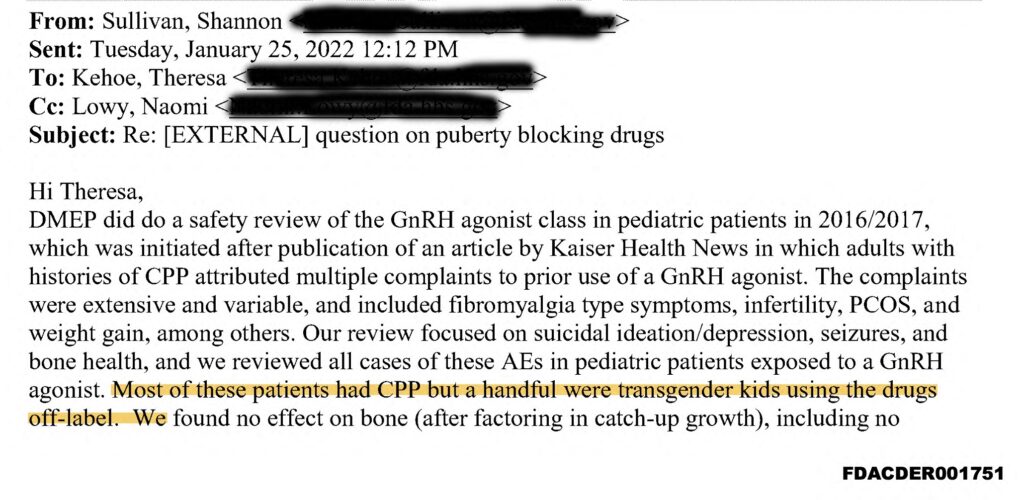
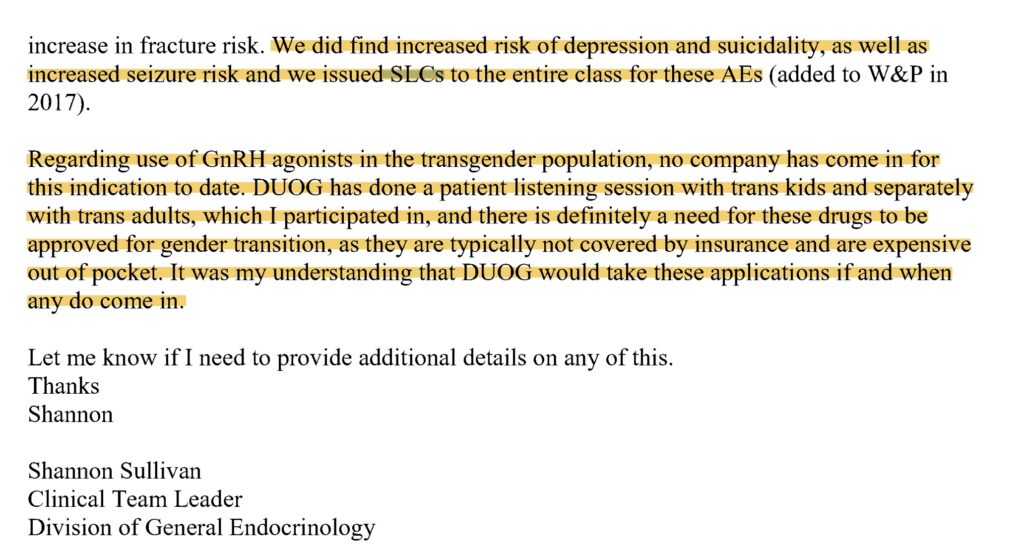














.jpg)








You must be logged in to post a comment.